Sometimes people call diabetes “a touch of sugar” or “borderline diabetes.” These terms suggest that someone doesn’t really have diabetes or has a less serious case, but every case of diabetes is serious.
What is Diabetes?
Diabetes is a disease that occurs when your blood glucose, also called blood sugar, is too high. Blood glucose is your main source of energy and comes from the food you eat. Insulin, a hormone made by the pancreas, helps glucose from food get into your cells to be used for energy. Sometimes your body doesn’t make enough—or any—insulin or doesn’t use insulin well. Glucose then stays in your blood and doesn’t reach your cells.
Over time, having too much glucose in your blood can cause health problems. Although diabetes has no cure, you can take steps to manage your diabetes and stay healthy.
Sometimes people call diabetes “a touch of sugar” or “borderline diabetes.” These terms suggest that someone doesn’t really have diabetes or has a less serious case, but every case of diabetes is serious.
What are the different types of diabetes?
The most common types of diabetes are type 1, type 2, and gestational diabetes.
Type 1 diabetes
If you have type 1 diabetes, your body does not make insulin. Your immune system attacks and destroys the cells in your pancreas that make insulin. Type 1 diabetes is usually diagnosed in children and young adults, although it can appear at any age. People with type 1 diabetes need to take insulin every day to stay alive.
Type 2 diabetes
If you have type 2 diabetes, your body does not make or use insulin well. You can develop type 2 diabetes at any age, even during childhood. However, this type of diabetes occurs most often in middle-aged and older people. Type 2 is the most common type of diabetes.
Gestational diabetes
Gestational diabetes develops in some women when they are pregnant. Most of the time, this type of diabetes goes away after the baby is born. However, if you’ve had gestational diabetes, you have a greater chance of developing type 2 diabetes later in life. Sometimes diabetes diagnosed during pregnancy is actually type 2 diabetes.
As of 2015, 30.3 million people in the United States, or 9.4 percent of the population, had diabetes. More than 1 in 4 of them didn’t know they had the disease. Diabetes affects 1 in 4 people over the age of 65. About 90-95 percent of cases in adults are type 2 diabetes.
Who is more likely to develop type 2 diabetes?
You are more likely to develop type 2 diabetes if you are age 45 or older, have a family history of diabetes, or are overweight. Physical inactivity, race, and certain health problems such as high blood pressure also affect your chance of developing type 2 diabetes. You are also more likely to develop type 2 diabetes if you have prediabetes or had gestational diabetes when you were pregnant. Learn more about risk factors for type 2 diabetes.
What health problems can people with diabetes develop?
Over time, high blood glucose leads to problems such as
Symptoms of type 1 diabetes can start quickly, in a matter of weeks. Symptoms of type 2 diabetes often develop slowly—over the course of several years—and can be so mild that you might not even notice them. Many people with type 2 diabetes have no symptoms. Some people do not find out they have the disease until they have diabetes-related health problems, such as blurred vision or heart trouble.
What causes type 1 diabetes?
Type 1 diabetes occurs when your immune system, the body’s system for fighting infection, attacks and destroys the insulin-producing beta cells of the pancreas. Scientists think type 1 diabetes is caused by genes and environmental factors, such as viruses, that might trigger the disease. Studies such as TrialNet are working to pinpoint causes of type 1 diabetes and possible ways to prevent or slow the disease.
What causes type 2 diabetes?
Type 2 diabetes—the most common form of diabetes—is caused by several factors, including lifestyle factors and genes.
Overweight, obesity, and physical inactivity
You are more likely to develop type 2 diabetes if you are not physically active and are overweight or obese. Extra weight sometimes causes insulin resistance and is common in people with type 2 diabetes. The location of body fat also makes a difference. Extra belly fat is linked to insulin resistance, type 2 diabetes, and heart and blood vessel disease. To see if your weight puts you at risk for type 2 diabetes, check out these Body Mass Index (BMI) charts.
Insulin resistance
Type 2 diabetes usually begins with insulin resistance, a condition in which muscle, liver, and fat cells do not use insulin well. As a result, your body needs more insulin to help glucose enter cells. At first, the pancreas makes more insulin to keep up with the added demand. Over time, the pancreas can’t make enough insulin, and blood glucose levels rise.
Genes and family history
As in type 1 diabetes, certain genes may make you more likely to develop type 2 diabetes. The disease tends to run in families and occurs more often in these racial/ethnic groups:
African Americans
Alaska Natives
American Indians
Asian Americans
Hispanics/Latinos
Native Hawaiians
Pacific Islanders
Genes also can increase the risk of type 2 diabetes by increasing a person’s tendency to become overweight or obese.
What causes gestational diabetes?
Scientists believe gestational diabetes, a type of diabetes that develops during pregnancy, is caused by the hormonal changes of pregnancy along with genetic and lifestyle factors.
Insulin resistance
Hormones produced by the placenta contribute to insulin resistance, which occurs in all women during late pregnancy. Most pregnant women can produce enough insulin to overcome insulin resistance, but some cannot. Gestational diabetes occurs when the pancreas can’t make enough insulin.
As with type 2 diabetes, extra weight is linked to gestational diabetes. Women who are overweight or obese may already have insulin resistance when they become pregnant. Gaining too much weight during pregnancy may also be a factor.
Hormonal changes, extra weight, and family history can contribute to gestational diabetes.
Genes and family history
Having a family history of diabetes makes it more likely that a woman will develop gestational diabetes, which suggests that genes play a role. Genes may also explain why the disorder occurs more often in African Americans, American Indians, Asians, and Hispanics/Latinas.
What else can cause diabetes?
Genetic mutations , other diseases, damage to the pancreas, and certain medicines may also cause diabetes.
Genetic mutations
Monogenic diabetes is caused by mutations, or changes, in a single gene. These changes are usually passed through families, but sometimes the gene mutation happens on its own. Most of these gene mutations cause diabetes by making the pancreas less able to make insulin. The most common types of monogenic diabetes are neonatal diabetes and maturity-onset diabetes of the young (MODY). Neonatal diabetes occurs in the first 6 months of life. Doctors usually diagnose MODY during adolescence or early adulthood, but sometimes the disease is not diagnosed until later in life.
Cystic fibrosis produces thick mucus that causes scarring in the pancreas. This scarring can prevent the pancreas from making enough insulin.
Hemochromatosis causes the body to store too much iron. If the disease is not treated, iron can build up in and damage the pancreas and other organs.
Hormonal diseases
Some hormonal diseases cause the body to produce too much of certain hormones, which sometimes cause insulin resistance and diabetes.
Acromegaly occurs when the body produces too much growth hormone.
Hyperthyroidism occurs when the thyroid gland produces too much thyroid hormone.
Damage to or removal of the pancreas
Pancreatitis, pancreatic cancer, and trauma can all harm the beta cells or make them less able to produce insulin, resulting in diabetes. If the damaged pancreas is removed, diabetes will occur due to the loss of the beta cells.
Medicines
Sometimes certain medicines can harm beta cells or disrupt the way insulin works. These include
niacin, a type of vitamin B3
certain types of diuretics, also called water pills
anti-seizure drugs
psychiatric drugs
drugs to treat human immunodeficiency virus (HIV )
anti-rejection medicines, used to help stop the body from rejecting a transplanted organ
Statins, which are medicines to reduce LDL (“bad”) cholesterol levels, can slightly increase the chance that you’ll develop diabetes. However, statins help protect you from heart disease and stroke. For this reason, the strong benefits of taking statins outweigh the small chance that you could develop diabetes.
If you take any of these medicines and are concerned about their side effects, talk with your doctor.
Risk Factors for Type 2 Diabetes
Your chances of developing type 2 diabetes depend on a combination of risk factors such as your genes and lifestyle. Although you can’t change risk factors such as family history, age, or ethnicity, you can change lifestyle risk factors around eating, physical activity, and weight. These lifestyle changes can affect your chances of developing type 2 diabetes.
Read about risk factors for type 2 diabetes below and see which ones apply to you. Taking action on the factors you can change can help you delay or prevent type 2 diabetes.
You are more likely to develop type 2 diabetes if you
have acanthosis nigricans—dark, thick, and velvety skin around your neck or armpits
You can also take the Diabetes Risk Test to learn about your risk for type 2 diabetes.
To see if your weight puts you at risk for type 2 diabetes, find your height in the Body Mass Index (BMI) charts below. If your weight is equal to or more than the weight listed, you have a greater chance of developing the disease.
If you are not Asian American or Pacific Islander
If you are Asian American
If you are Pacific Islander
At-risk BMI ≥ 25
At-risk BMI ≥ 23
At-risk BMI ≥ 26
Height
Weight
Height
Weight
Height
Weight
4'10"
119
4'10"
110
4'10"
124
4'11"
124
4'11"
114
4'11"
128
5'0"
128
5'0"
118
5'0"
133
5'1"
132
5'1"
122
5'1"
137
5'2"
136
5'2"
126
5'2"
142
5'3"
141
5'3"
130
5'3"
146
5'4"
145
5'4"
134
5'4"
151
5'5"
150
5'5"
138
5'5"
156
5'6"
155
5'6"
142
5'6"
161
5'7"
159
5'7"
146
5'7"
166
5'8"
164
5'8"
151
5'8"
171
5'9"
169
5'9"
155
5'9"
176
5'10"
174
5'10"
160
5'10"
181
5'11"
179
5'11"
165
5'11"
186
6'0"
184
6'0"
169
6'0"
191
6'1"
189
6'1"
174
6'1"
197
6'2"
194
6'2"
179
6'2"
202
6'3"
200
6'3"
184
6'3"
208
6'4"
205
6'4"
189
6'4"
213
What can I do to prevent type 2 diabetes?
You can take steps to help prevent or delay type 2 diabetes by losing weight if you are overweight, eating fewer calories, and being more physically active. Talk with your health care professional about any of the health conditions listed above that may require medical treatment. Managing these health problems may help reduce your chances of developing type 2 diabetes. Also, ask your health care professional about any medicines you take that might increase your risk.
Preventing Type 2 Diabetes
Perhaps you have learned that you have a high chance of developing type 2 diabetes, the most common type of diabetes. You might be overweight or have a parent, brother, or sister with type 2 diabetes. Maybe you had gestational diabetes, which is diabetes that develops during pregnancy. These are just a few examples of factors that can raise your chances of developing type 2 diabetes.
Diabetes can cause serious health problems, such as heart disease, stroke, and eye and foot problems. Prediabetes also can cause health problems. The good news is that type 2 diabetes can be delayed or even prevented. The longer you have diabetes, the more likely you are to develop health problems, so delaying diabetes by even a few years will benefit your health. You can help prevent or delay type 2 diabetes by losing a modest amount of weight by following a reduced-calorie eating plan and being physically active most days of the week. Ask your doctor if you should take the diabetes drug metformin to help prevent or delay type 2 diabetes.1
How can I lower my chances of developing type 2 diabetes?
Research such as the Diabetes Prevention Program shows that you can do a lot to reduce your chances of developing type 2 diabetes. Here are some things you can change to lower your risk:
Lose weight and keep it off. You may be able to prevent or delay diabetes by losing 5 to 7 percent of your starting weight.1 For instance, if you weigh 200 pounds, your goal would be to lose about 10 to 14 pounds.
Move more. Get at least 30 minutes of physical activity 5 days a week. If you have not been active, talk with your health care professional about which activities are best. Start slowly to build up to your goal.
Eat healthy foods most of the time. Eat smaller portions to reduce the amount of calories you eat each day and help you lose weight. Choosing foods with less fat is another way to reduce calories. Drink water instead of sweetened beverages.
Ask your health care professional about what other changes you can make to prevent or delay type 2 diabetes.
Most often, your best chance for preventing type 2 diabetes is to make lifestyle changes that work for you long term. Get started with Your Game Plan to Prevent Type 2 Diabetes.
Losing weight through healthy eating and regular physical activity can help you prevent type 2 diabetes.
What should I do if my health care professional told me I have prediabetes?
Prediabetes is when your blood glucose, also called blood sugar, levels are higher than normal, but not high enough to be called diabetes. Having prediabetes is serious because it raises your chance of developing type 2 diabetes. Many of the same factors that raise your chance of developing type 2 diabetes put you at risk for prediabetes.
Other names for prediabetes include impaired fasting glucose or impaired glucose tolerance. Some people call prediabetes “borderline diabetes.”
About 1 in 3 Americans has prediabetes, according to recent diabetes statistics from the Centers for Disease Control and Prevention. You won’t know if you have prediabetes unless you are tested.
If you have prediabetes, you can lower your chance of developing type 2 diabetes. Lose weight if you need to, become more physically active, and follow a reduced-calorie eating plan.
Being physically active is one way to help prevent prediabetes from progressing to type 2 diabetes.
If I had gestational diabetes when I was pregnant, how can I lower my chances of developing type 2 diabetes?
Gestational diabetes is a type of diabetes that develops during pregnancy. Most of the time, gestational diabetes goes away after your baby is born. Even if your gestational diabetes goes away, you still have a greater chance of developing type 2 diabetes within 5 to 10 years. Your child may also be more likely to become obese and develop type 2 diabetes later in life. Making healthy choices helps the whole family and may protect your child from becoming obese or developing diabetes.
Being physically active together is a great way to lower your own and your child’s chance of developing type 2 diabetes.
Here are steps you should take for yourself and your child if you had gestational diabetes:
Get tested for diabetes 6 to 12 weeks after your baby is born. If your blood glucose is still high, you may have type 2 diabetes. If your blood glucose is normal, you should get tested every 3 years to see if you have developed type 2 diabetes.
Be more active and make healthy food choices to get back to a healthy weight.
Breastfeed your baby. Breastfeeding gives your baby the right balance of nutrients and helps you burn calories.
Ask your doctor if you should take the diabetes drug metformin to help prevent type 2 diabetes.1
Diabetes Tests & Diagnosis
Your health care professional can diagnose diabetes, prediabetes, and gestational diabetes through blood tests. The blood tests show if your blood glucose, also called blood sugar, is too high.
Do not try to diagnose yourself if you think you might have diabetes. Testing equipment that you can buy over the counter, such as a blood glucose meter, cannot diagnose diabetes.
Who should be tested for diabetes?
Anyone who has symptoms of diabetes should be tested for the disease. Some people will not have any symptoms but may have risk factors for diabetes and need to be tested. Testing allows health care professionals to find diabetes sooner and work with their patients to manage diabetes and prevent complications.
Testing also allows health care professionals to find prediabetes. Making lifestyle changes to lose a modest amount of weight if you are overweight may help you delay or prevent type 2 diabetes.
Blood tests help health care professionals diagnose diabetes and prediabetes.
Type 1 diabetes
Most often, testing for type 1 diabetes occurs in people with diabetes symptoms. Doctors usually diagnose type 1 diabetes in children and young adults. Because type 1 diabetes can run in families, a study called TrialNet offers free testing to family members of people with the disease, even if they don’t have symptoms.
Type 2 diabetes
Experts recommend routine testing for type 2 diabetes if you
are age 45 or older
are between the ages of 19 and 44, are overweight or obese, and have one or more other diabetes risk factors
are a woman who had gestational diabetes1
Medicare covers the cost of diabetes tests for people with certain risk factors for diabetes. If you have Medicare, find out if you qualify for coverage . If you have different insurance, ask your insurance company if it covers diabetes tests.
Though type 2 diabetes most often develops in adults, children also can develop type 2 diabetes. Experts recommend testing children between the ages of 10 and 18 who are overweight or obese and have at least two other risk factors for developing diabetes.1
low birthweight
a mother who had diabetes while pregnant with them
All pregnant women who do not have a prior diabetes diagnosis should be tested for gestational diabetes. If you are pregnant, you will take a glucose challenge test between 24 and 28 weeks of pregnancy.1
What tests are used to diagnose diabetes and prediabetes?
Health care professionals most often use the fasting plasma glucose (FPG) test or the A1C test to diagnose diabetes. In some cases, they may use a random plasma glucose (RPG) test.
Fasting plasma glucose (FPG) test
The FPG blood test measures your blood glucose level at a single point in time. For the most reliable results, it is best to have this test in the morning, after you fast for at least 8 hours. Fasting means having nothing to eat or drink except sips of water.
A1C test
The A1C test is a blood test that provides your average levels of blood glucose over the past 3 months. Other names for the A1C test are hemoglobin A1C, HbA1C, glycated hemoglobin, and glycosylated hemoglobin test. You can eat and drink before this test. When it comes to using the A1C to diagnose diabetes, your doctor will consider factors such as your age and whether you have anemia or another problem with your blood.1 The A1C test is not accurate in people with anemia.
Your health care professional will report your A1C test result as a percentage, such as an A1C of 7 percent. The higher the percentage, the higher your average blood glucose levels.
People with diabetes also use information from the A1C test to help manage their diabetes.
Random plasma glucose (RPG) test
Sometimes health care professionals use the RPG test to diagnose diabetes when diabetes symptoms are present and they do not want to wait until you have fasted. You do not need to fast overnight for the RPG test. You may have this blood test at any time.
What tests are used to diagnose gestational diabetes?
Pregnant women may have the glucose challenge test, the oral glucose tolerance test, or both. These tests show how well your body handles glucose.
Glucose challenge test
If you are pregnant and a health care professional is checking you for gestational diabetes, you may first receive the glucose challenge test. Another name for this test is the glucose screening test. In this test, a health care professional will draw your blood 1 hour after you drink a sweet liquid containing glucose. You do not need to fast for this test. If your blood glucose is too high—135 to 140 or more—you may need to return for an oral glucose tolerance test while fasting.
Oral glucose tolerance test (OGTT)
The OGTT measures blood glucose after you fast for at least 8 hours. First, a health care professional will draw your blood. Then you will drink the liquid containing glucose. For diagnosing gestational diabetes, you will need your blood drawn every hour for 2 to 3 hours.
High blood glucose levels at any two or more blood test times during the OGTT—fasting, 1 hour, 2 hours, or 3 hours—mean you have gestational diabetes. Your health care team will explain what your OGTT results mean.
Health care professionals also can use the OGTT to diagnose type 2 diabetes and prediabetes in people who are not pregnant. The OGTT helps health care professionals detect type 2 diabetes and prediabetes better than the FPG test. However, the OGTT is a more expensive test and is not as easy to give. To diagnose type 2 diabetes and prediabetes, a health care professional will need to draw your blood 1 hour after you drink the liquid containing glucose and again after 2 hours.
What test numbers tell me if I have diabetes or prediabetes?
Each test to detect diabetes and prediabetes uses a different measurement. Usually, the same test method needs to be repeated on a second day to diagnose diabetes. Your doctor may also use a second test method to confirm that you have diabetes.
The following table helps you understand what your test numbers mean if you are not pregnant.
Diagnosis
A1C (percent)
Fasting plasma glucose (FPG)a
Oral glucose tolerance test (OGTT)ab
Random plasma glucose test (RPG)a
Normal
below 5.7
99 or below
139 or below
Prediabetes
5.7 to 6.4
100 to 125
140 to 199
Diabetes
6.5 or above
126 or above
200 or above
200 or above
Which tests help my health care professional know what kind of diabetes I have?
Even though the tests described here can confirm that you have diabetes, they can’t identify what type you have. Sometimes health care professionals are unsure if diabetes is type 1 or type 2. A rare type of diabetes that can occur in babies, called monogenic diabetes, can also be mistaken for type 1 diabetes. Treatment depends on the type of diabetes, so knowing which type you have is important.
To find out if your diabetes is type 1, your health care professional may look for certain autoantibodies. Autoantibodies are antibodies that mistakenly attack your healthy tissues and cells. The presence of one or more of several types of autoantibodies specific to diabetes is common in type 1 diabetes, but not in type 2 or monogenic diabetes. A health care professional will have to draw your blood for this test.
If you had diabetes while you were pregnant, you should get tested no later than 12 weeks after your baby is born to see if you have type 2 diabetes.
Managing Diabetes
You can manage your diabetes and live a long and healthy life by taking care of yourself each day.
Diabetes can affect almost every part of your body. Therefore, you will need to manage your blood glucose levels, also called blood sugar. Managing your blood glucose, as well as your blood pressure and cholesterol, can help prevent the health problems that can occur when you have diabetes.
How can I manage my diabetes?
With the help of your health care team, you can create a diabetes self-care plan to manage your diabetes. Your self-care plan may include these steps:
Manage your diabetes ABCs
Knowing your diabetes ABCs will help you manage your blood glucose, blood pressure, and cholesterol. Stopping smoking if you smoke will also help you manage your diabetes. Working toward your ABC goals can help lower your chances of having a heart attack, stroke, or other diabetes problems.
A for the A1C test
The A1C test shows your average blood glucose level over the past 3 months. The A1C goal for many people with diabetes is below 7 percent. Ask your health care team what your goal should be.
B for Blood pressure
The blood pressure goal for most people with diabetes is below 140/90 mm Hg. Ask what your goal should be.
C for Cholesterol
You have two kinds of cholesterol in your blood: LDL and HDL. LDL or “bad” cholesterol can build up and clog your blood vessels. Too much bad cholesterol can cause a heart attack or stroke. HDL or “good” cholesterol helps remove the “bad” cholesterol from your blood vessels.
Ask your health care team what your cholesterol numbers should be. If you are over 40 years of age, you may need to take a statin drug for heart health.
S for Stop smoking
Not smoking is especially important for people with diabetes because both smoking and diabetes narrow blood vessels. Blood vessel narrowing makes your heart work harder. E-cigarettes aren’t a safe option either.
If you quit smoking
you will lower your risk for heart attack, stroke, nerve disease, kidney disease, diabetic eye disease, and amputation
your cholesterol and blood pressure levels may improve
your blood circulation will improve
you may have an easier time being physically active
If you smoke or use other tobacco products, stop. Ask for help so you don’t have to do it alone. You can start by calling the national quitline at 1-800-QUITNOW or 1-800-784-8669. For tips on quitting, go to SmokeFree.gov .
Keeping your A1C, blood pressure, and cholesterol levels close to your goals and stopping smoking may help prevent the long-term harmful effects of diabetes. These health problems include heart disease, stroke, kidney disease, nerve damage, and eye disease. You can keep track of your ABCs with a diabetes care record(PDF, 568 KB). Take it with you on your health care visits. Talk about your goals and how you are doing, and whether you need to make any changes in your diabetes care plan.
Follow your diabetes meal plan
Make a diabetes meal plan with help from your health care team. Following a meal plan will help you manage your blood glucose, blood pressure, and cholesterol.
Choose fruits and vegetables, beans, whole grains, chicken or turkey without the skin, fish, lean meats, and nonfat or low-fat milk and cheese. Drink water instead of sugar-sweetened beverages. Choose foods that are lower in calories, saturated fat, trans fat, sugar, and salt. Learn more about eating, diet, and nutrition with diabetes.
Make physical activity part of your daily routine
Set a goal to be more physically active. Try to work up to 30 minutes or more of physical activity on most days of the week.
Brisk walking and swimming are good ways to move more. If you are not active now, ask your health care team about the types and amounts of physical activity that are right for you. Learn more about being physically active with diabetes.
Swimming or water walking is a good way to move more.
Following your meal plan and being more active can help you stay at or get to a healthy weight. If you are overweight or obese, work with your health care team to create a weight-loss plan that is right for you.
Take your medicine
Take your medicines for diabetes and any other health problems, even when you feel good or have reached your blood glucose, blood pressure, and cholesterol goals. These medicines help you manage your ABCs. Ask your doctor if you need to take aspirin to prevent a heart attack or stroke. Tell your health care professional if you cannot afford your medicines or if you have any side effects from your medicines. Learn more about insulin and other diabetes medicines.
Check your blood glucose levels
For many people with diabetes, checking their blood glucose level each day is an important way to manage their diabetes. Monitoring your blood glucose level is most important if you take insulin. The results of blood glucose monitoring can help you make decisions about food, physical activity, and medicines.
Checking and recording your blood glucose level is an important part of managing diabetes.
The most common way to check your blood glucose level at home is with a blood glucose meter. You get a drop of blood by pricking the side of your fingertip with a lancet. Then you apply the blood to a test strip. The meter will show you how much glucose is in your blood at the moment.
Ask your health care team how often you should check your blood glucose levels. Make sure to keep a record of your blood glucose self-checks. You can print copies of this glucose self-check chart(PDF, 2 MB). Take these records with you when you visit your health care team.
What is continuous glucose monitoring?
Continuous glucose monitoring (CGM) is another way to check your glucose levels. Most CGM systems use a tiny sensor that you insert under your skin. The sensor measures glucose levels in the fluids between your body’s cells every few minutes and can show changes in your glucose level throughout the day and night. If the CGM system shows that your glucose is too high or too low, you should check your glucose with a blood glucose meter before making any changes to your eating plan, physical activity, or medicines. A CGM system is especially useful for people who use insulin and have problems with low blood glucose.
What are the recommended targets for blood glucose levels?
Many people with diabetes aim to keep their blood glucose at these normal levels:
Before a meal: 80 to 130 mg/dL
About 2 hours after a meal starts: less than 180 mg/dL
Talk with your health care team about the best target range for you. Be sure to tell your health care professional if your glucose levels often go above or below your target range.
What happens if my blood glucose level becomes too low?
Sometimes blood glucose levels drop below where they should be, which is called hypoglycemia. For most people with diabetes, the blood glucose level is too low when it is below 70 mg/dL.
What happens if my blood glucose level becomes too high?
Doctors call high blood glucose hyperglycemia.
Symptoms that your blood glucose levels may be too high include
feeling thirsty
feeling tired or weak
headaches
urinating often
blurred vision
If you often have high blood glucose levels or symptoms of high blood glucose, talk with your health care team. You may need a change in your diabetes meal plan, physical activity plan, or medicines.
Work with your health care team
Most people with diabetes get health care from a primary care professional. Primary care professionals include internists, family physicians, and pediatricians. Sometimes physician assistants and nurses with extra training, called nurse practitioners, provide primary care. You also will need to see other care professionals from time to time. A team of health care professionals can help you improve your diabetes self-care. Remember, you are the most important member of your health care team.
Besides a primary care professional, your health care team may include
When you see your doctor, review your diabetes self-care plan and blood glucose chart.
You should see your health care team at least twice a year, and more often if you are having problems or are having trouble reaching your blood glucose, blood pressure, or cholesterol goals. At each visit, be sure you have a blood pressure check, foot check, and weight check; and review your self-care plan. Talk with your health care team about your medicines and whether you need to adjust them. Routine health care will help you find and treat any health problems early, or may be able to help prevent them.
Feeling stressed, sad, or angry is common when you live with diabetes. Stress can raise your blood glucose levels, but you can learn ways to lower your stress. Try deep breathing, gardening, taking a walk, doing yoga, meditating, doing a hobby, or listening to your favorite music. Consider taking part in a diabetes education program or support group that teaches you techniques for managing stress. Learn more about healthy ways to cope with stress .
Depression is common among people with a chronic, or long-term, illness . Depression can get in the way of your efforts to manage your diabetes. Ask for help if you feel down. A mental health counselor, support group, clergy member, friend, or family member who will listen to your feelings may help you feel better.
Try to get 7 to 8 hours of sleep each night. Getting enough sleep can help improve your mood and energy level. You can take steps to improve your sleep habits . If you often feel sleepy during the day, you may have obstructive sleep apnea , a condition in which your breathing briefly stops many times during the night. Sleep apnea is common in people who have diabetes. Talk with your health care team if you think you have a sleep problem.
Remember, managing diabetes isn’t easy, but it’s worth it.
Insulin, Medicines, & Other Diabetes Treatments
Taking insulin or other diabetes medicines is often part of treating diabetes. Along with healthy food choices and physical activity, medicine can help you manage the disease. Some other treatment options are also available.
What medicines might I take for diabetes?
The medicine you take will vary by your type of diabetes and how well the medicine controls your blood glucose levels, also called blood sugar. Other factors, such as your other health conditions, medication costs, and your daily schedule may play a role in what diabetes medicine you take.
Type 1 diabetes
If you have type 1 diabetes, you must take insulin because your body no longer makes this hormone. You will need to take insulin several times during the day, including with meals. You also could use an insulin pump, which gives you small, steady doses throughout the day.
Type 2 diabetes
Some people with type 2 diabetes can manage their disease by making healthy food choices and being more physically active. Many people with type 2 diabetes need diabetes medicines as well. These medicines may include diabetes pills or medicines you inject under your skin, such as insulin. In time, you may need more than one diabetes medicine to control your blood glucose. Even if you do not take insulin, you may need it at special times, such as during pregnancy or if you are in the hospital.
Gestational diabetes
If you have gestational diabetes, you should first try to control your blood glucose level by making healthy food choices and getting regular physical activity. If you can’t reach your blood glucose target, your health care team will talk with you about diabetes medicines, such as insulin or the diabetes pill metformin, that may be safe for you to take during pregnancy. Your health care team may start you on diabetes medicines right away if your blood glucose is very high.
No matter what type of diabetes you have, taking diabetes medicines every day can feel like a burden sometimes. You may also need medicines for other health problems, such as high blood pressure or high cholesterol, as part of your diabetes care plan. View resources that may help you manage your medication plan.
What are the different types of insulin?
Several types of insulin are available. Each type starts to work at a different speed, known as “onset,” and its effects last a different length of time, known as “duration.” Most types of insulin reach a peak, which is when they have the strongest effect. Then the effects of the insulin wear off over the next few hours or so.
The chart above gives averages. Follow your doctor’s advice on when and how to take your insulin. Your doctor might also recommend premixed insulin, which is a mix of two types of insulin. Some types of insulin cost more than others, so talk with your doctor about your options if you're concerned about cost. Read about financial help for diabetes care.
What are the different ways to take insulin?
The way you take insulin may depend on your lifestyle, insurance plan, and preferences. You may decide that needles are not for you and prefer a different method. Talk with your doctor about the options and which is best for you. Most people with diabetes use a needle and syringe, pen, or insulin pump. Inhalers, injection ports, and jet injectors are less common.
Needle and syringe
You’ll give yourself insulin shots using a needle and syringe. You will draw up your dose of insulin from the vial, or bottle, into the syringe. Insulin works fastest when you inject it in your belly, but you should rotate spots where you inject insulin. Other injection spots include your thigh, buttocks, or upper arm. Some people with diabetes who take insulin need two to four shots a day to reach their blood glucose targets. Others can take a single shot.
Insulin shots involve drawing insulin from a vial into a syringe and then injecting it under your skin.
Pen
An insulin pen looks like a pen but has a needle for its point. Some insulin pens come filled with insulin and are disposable. Others have room for an insulin cartridge that you insert and then replace after use. Insulin pens cost more than needles and syringes but many people find them easier to use.
An insulin pen is a convenient way to take insulin
Pump
An insulin pump is a small machine that gives you small, steady doses of insulin throughout the day. You wear one type of pump outside your body on a belt or in a pocket or pouch. The insulin pump connects to a small plastic tube and a very small needle. You insert the needle under your skin and it stays in place for several days. Insulin then pumps from the machine through the tube into your body 24 hours a day. You also can give yourself doses of insulin through the pump at mealtimes. Another type of pump has no tubes and attaches directly to your skin, such as a self-adhesive pod.
Insulin pumps deliver insulin 24 hours a day.
Inhaler
Another way to take insulin is by breathing powdered insulin from an inhaler device into your mouth. The insulin goes into your lungs and moves quickly into your blood. Inhaled insulin is only for adults with type 1 or type 2 diabetes.
Injection port
An injection port has a short tube that you insert into the tissue beneath your skin. On the skin’s surface, an adhesive patch or dressing holds the port in place. You inject insulin through the port with a needle and syringe or an insulin pen. The port stays in place for a few days, and then you replace the port. With an injection port, you no longer puncture your skin for each shot—only when you apply a new port.
Jet injector
This device sends a fine spray of insulin into the skin at high pressure instead of using a needle to deliver the insulin.
What oral medicines treat type 2 diabetes?
You may need medicines along with healthy eating and physical activity habits to manage your type 2 diabetes. You can take many diabetes medicines by mouth. These medicines are called oral medicines.
Most people with type 2 diabetes start medical treatment with metformin pills. Metformin also comes as a liquid. Metformin lowers the amount of glucose that your liver makes and helps your body use insulin better. This drug may help you lose a small amount of weight.
Other oral medicines act in different ways to lower blood glucose levels. You may need to add another diabetes medicine after a while or use a combination treatment. Combining two or three kinds of diabetes medicines can lower blood glucose levels more than taking just one.
Read about different kinds of diabetes medicines from the Food and Drug Administration (FDA).
What other injectable medicines treat type 2 diabetes?
Besides insulin, other types of injected medicines are available. These medicines help keep your blood glucose level from going too high after you eat. They may make you feel less hungry and help you lose some weight. Other injectable medicines are not substitutes for insulin. Learn more about noninsulin injectable medicines .
What should I know about side effects of diabetes medicines?
Side effects are problems that result from a medicine. Some diabetes medicines can cause hypoglycemia, also called low blood glucose, if you don’t balance your medicines with food and activity.
Ask your doctor whether your diabetes medicine can cause hypoglycemia or other side effects, such as upset stomach and weight gain. Take your diabetes medicines as your health care professional has instructed you, to help prevent side effects and diabetes problems.
Do I have other treatment options for my diabetes?
When medicines and lifestyle changes are not enough to manage your diabetes, a less common treatment may be an option. Other treatments include bariatric surgery for certain people with type 1 or type 2 diabetes, and an "artificial pancreas" and pancreatic islet transplantation for some people with type 1 diabetes.
Bariatric surgery
Also called weight-loss surgery or metabolic surgery, bariatric surgery may help some people with obesity and type 2 diabetes lose a large amount of weight and regain normal blood glucose levels. Some people with diabetes may no longer need their diabetes medicine after bariatric surgery. Whether and for how long blood glucose levels improve seems to vary by the patient, type of weight-loss surgery, and amount of weight the person loses. Other factors include how long someone has had diabetes and whether or not the person uses insulin.1
Recent research suggests that weight-loss surgery also may help improve blood glucose control in people with type 1 diabetes who are obese.2
Researchers are studying the long-term results of bariatric surgery in people with type 1 and type 2 diabetes.
Artificial Pancreas
The NIDDK has played an important role in developing “artificial pancreas” technology. An artificial pancreas replaces manual blood glucose testing and the use of insulin shots or a pump. A single system monitors blood glucose levels around the clock and provides insulin or a combination of insulin and a second hormone, glucagon, automatically. The system can also be monitored remotely, for example by parents or medical staff.
In 2016, the FDA approved a type of artificial pancreas system called a hybrid closed-loop system. This system tests your glucose level every 5 minutes throughout the day and night, and automatically gives you the right amount of insulin.
You still need to manually adjust the amount of insulin the pump delivers at mealtimes. But, the artificial pancreas may free you from some of the daily tasks needed to keep your blood glucose stable—or help you sleep through the night without the need to wake and test your glucose or take medicine.
The hybrid closed-loop system is expected to be available in the U.S. in 2017. Talk with your health care provider about whether this system might be right for you.
The NIDDK has funded several important studies on different types of artificial pancreas devices to better help people with type 1 diabetes manage their disease. The devices may also help people with type 2 diabetes and gestational diabetes.
Pancreatic islet transplantation
Pancreatic islet transplantation is an experimental treatment for poorly controlled type 1 diabetes. Pancreatic islets are clusters of cells in the pancreas that make the hormone insulin. In type 1 diabetes, the body’s immune system attacks these cells. A pancreatic islet transplant replaces destroyed islets with new ones that make and release insulin. This procedure takes islets from the pancreas of an organ donor and transfers them to a person with type 1 diabetes. Because researchers are still studying pancreatic islet transplantation, the procedure is only available to people enrolled in research studies. Learn more about islet transplantation studies .
Diabetes Diet, Eating, & Physical Activity
Nutrition and physical activity are important parts of a healthy lifestyle when you have diabetes. Along with other benefits, following a healthy meal plan and being active can help you keep your blood glucose level, also called blood sugar, in your target range. To manage your blood glucose, you need to balance what you eat and drink with physical activity and diabetes medicine, if you take any. What you choose to eat, how much you eat, and when you eat are all important in keeping your blood glucose level in the range that your health care team recommends.
Becoming more active and making changes in what you eat and drink can seem challenging at first. You may find it easier to start with small changes and get help from your family, friends, and health care team.
Eating well and being physically active most days of the week can help you
keep your blood glucose level, blood pressure, and cholesterol in your target ranges
You may worry that having diabetes means going without foods you enjoy. The good news is that you can still eat your favorite foods, but you might need to eat smaller portions or enjoy them less often. Your health care team will help create a diabetes meal plan for you that meets your needs and likes.
The key to eating with diabetes is to eat a variety of healthy foods from all food groups, in the amounts your meal plan outlines.
The food groups are
vegetables
nonstarchy: includes broccoli, carrots, greens, peppers, and tomatoes
starchy: includes potatoes, corn, and green peas
fruits—includes oranges, melon, berries, apples, bananas, and grapes
grains—at least half of your grains for the day should be whole grains
includes wheat, rice, oats, cornmeal, barley, and quinoa
examples: bread, pasta, cereal, and tortillas
protein
lean meat
chicken or turkey without the skin
fish
eggs
nuts and peanuts
dried beans and certain peas, such as chickpeas and split peas
beverages with added sugars, such as juice, regular soda, and regular sports or energy drinks
Drink water instead of sweetened beverages. Consider using a sugar substitute in your coffee or tea.
If you drink alcohol, drink moderately—no more than one drink a day if you’re a woman or two drinks a day if you’re a man. If you use insulin or diabetes medicines that increase the amount of insulin your body makes, alcohol can make your blood glucose level drop too low. This is especially true if you haven’t eaten in a while. It’s best to eat some food when you drink alcohol.
When should I eat if I have diabetes?
Some people with diabetes need to eat at about the same time each day. Others can be more flexible with the timing of their meals. Depending on your diabetes medicines or type of insulin, you may need to eat the same amount of carbohydrates at the same time each day. If you take “mealtime” insulin, your eating schedule can be more flexible.
If you use certain diabetes medicines or insulin and you skip or delay a meal, your blood glucose level can drop too low. Ask your health care team when you should eat and whether you should eat before and after physical activity.
How much can I eat if I have diabetes?
Eating the right amount of food will also help you manage your blood glucose level and your weight. Your health care team can help you figure out how much food and how many calories you should eat each day.
Weight-loss planning
If you are overweight or have obesity, work with your health care team to create a weight-loss plan.
The Body Weight Planner can help you tailor your calorie and physical activity plans to reach and maintain your goal weight.
To lose weight, you need to eat fewer calories and replace less healthy foods with foods lower in calories, fat, and sugar.
Two common ways to help you plan how much to eat if you have diabetes are the plate method and carbohydrate counting, also called carb counting. Check with your health care team about the method that’s best for you.
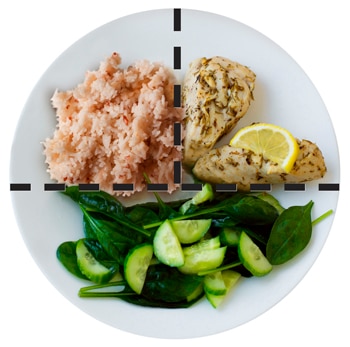
Plate method
The plate method helps you control your portion sizes. You don’t need to count calories. The plate method shows the amount of each food group you should eat. This method works best for lunch and dinner.
Use a 9-inch plate. Put nonstarchy vegetables on half of the plate; a meat or other protein on one-fourth of the plate; and a grain or other starch on the last one-fourth. Starches include starchy vegetables such as corn and peas. You also may eat a small bowl of fruit or a piece of fruit, and drink a small glass of milk as included in your meal plan.
The plate method shows the amount of each food group you should eat.
You can find many different combinations of food and more details about using the plate method from the American Diabetes Association’s Create Your Plate .
Your daily eating plan also may include small snacks between meals.
Portion sizes
You can use everyday objects or your hand to judge the size of a portion.
1 serving of meat or poultry is the palm of your hand or a deck of cards
1 3-ounce serving of fish is a checkbook
1 serving of cheese is six dice
1/2 cup of cooked rice or pasta is a rounded handful or a tennis ball
1 serving of a pancake or waffle is a DVD
2 tablespoons of peanut butter is a ping-pong ball
Carbohydrate counting
Carbohydrate counting involves keeping track of the amount of carbohydrates you eat and drink each day. Because carbohydrates turn into glucose in your body, they affect your blood glucose level more than other foods do. Carb counting can help you manage your blood glucose level. If you take insulin, counting carbohydrates can help you know how much insulin to take.
The right amount of carbohydrates varies by how you manage your diabetes, including how physically active you are and what medicines you take, if any. Your health care team can help you create a personal eating plan based on carbohydrate counting.
The amount of carbohydrates in foods is measured in grams. To count carbohydrate grams in what you eat, you’ll need to
learn which foods have carbohydrates
read the Nutrition Facts food label, or learn to estimate the number of grams of carbohydrate in the foods you eat
add the grams of carbohydrate from each food you eat to get your total for each meal and for the day
Most carbohydrates come from starches, fruits, milk, and sweets. Try to limit carbohydrates with added sugars or those with refined grains, such as white bread and white rice. Instead, eat carbohydrates from fruit, vegetables, whole grains, beans, and low-fat or nonfat milk.
Choose healthy carbohydrates, such as fruit, vegetables, whole grains, beans, and low-fat milk, as part of your diabetes meal plan.
In addition to using the plate method and carb counting, you may want to visit a registered dietitian (RD) for medical nutrition therapy.
What is medical nutrition therapy?
Medical nutrition therapy is a service provided by an RD to create personal eating plans based on your needs and likes. For people with diabetes, medical nutrition therapy has been shown to improve diabetes management. Medicare pays for medical nutrition therapy for people with diabetes. If you have insurance other than Medicare, ask if it covers medical nutrition therapy for diabetes.
Will supplements and vitamins help my diabetes?
No clear proof exists that taking dietary supplements such as vitamins, minerals, herbs, or spices can help manage diabetes.1 You may need supplements if you cannot get enough vitamins and minerals from foods. Talk with your health care provider before you take any dietary supplement since some can cause side effects or affect how your medicines work.2
Why should I be physically active if I have diabetes?
Physical activity is an important part of managing your blood glucose level and staying healthy. Being active has many health benefits.
burns extra calories so you can keep your weight down if needed
improves your mood
can prevent falls and improve memory in older adults
may help you sleep better
If you are overweight, combining physical activity with a reduced-calorie eating plan can lead to even more benefits. In the Look AHEAD: Action for Health in Diabetes study,1 overweight adults with type 2 diabetes who ate less and moved more had greater long-term health benefits compared to those who didn’t make these changes. These benefits included improved cholesterol levels, less sleep apnea, and being able to move around more easily.
Even small amounts of physical activity can help. Experts suggest that you aim for at least 30 minutes of moderate or vigorous physical activity 5 days of the week.3 Moderate activity feels somewhat hard, and vigorous activity is intense and feels hard. If you want to lose weight or maintain weight loss, you may need to do 60 minutes or more of physical activity 5 days of the week.3
Be patient. It may take a few weeks of physical activity before you see changes in your health.
How can I be physically active safely if I have diabetes?
Be sure to drink water before, during, and after exercise to stay well hydrated. The following are some other tips for safe physical activity when you have diabetes.
Drink water when you exercise to stay well hydrated.
Plan ahead
Talk with your health care team before you start a new physical activity routine, especially if you have other health problems. Your health care team will tell you a target range for your blood glucose level and suggest how you can be active safely.
Your health care team also can help you decide the best time of day for you to do physical activity based on your daily schedule, meal plan, and diabetes medicines. If you take insulin, you need to balance the activity that you do with your insulin doses and meals so you don’t get low blood glucose.
Prevent low blood glucose
Because physical activity lowers your blood glucose, you should protect yourself against low blood glucose levels, also called hypoglycemia. You are most likely to have hypoglycemia if you take insulin or certain other diabetes medicines, such as a sulfonylurea. Hypoglycemia also can occur after a long intense workout or if you have skipped a meal before being active. Hypoglycemia can happen during or up to 24 hours after physical activity.
Planning is key to preventing hypoglycemia. For instance, if you take insulin, your health care provider might suggest you take less insulin or eat a small snack with carbohydrates before, during, or after physical activity, especially intense activity.4
You may need to check your blood glucose level before, during, and right after you are physically active.
Take care of your feet
People with diabetes may have problems with their feet because of poor blood flow and nerve damage that can result from high blood glucose levels. To help prevent foot problems, you should wear comfortable, supportive shoes and take care of your feet before, during, and after physical activity.
What physical activities should I do if I have diabetes?
Most kinds of physical activity can help you take care of your diabetes. Certain activities may be unsafe for some people, such as those with low vision or nerve damage to their feet. Ask your health care team what physical activities are safe for you. Many people choose walking with friends or family members for their activity.
Doing different types of physical activity each week will give you the most health benefits. Mixing it up also helps reduce boredom and lower your chance of getting hurt. Try these options for physical activity.
Add extra activity to your daily routine
If you have been inactive or you are trying a new activity, start slowly, with 5 to 10 minutes a day. Then add a little more time each week. Increase daily activity by spending less time in front of a TV or other screen. Try these simple ways to add physical activities in your life each day:
Walk around while you talk on the phone or during TV commercials.
Do chores, such as work in the garden, rake leaves, clean the house, or wash the car.
Park at the far end of the shopping center parking lot and walk to the store.
Take the stairs instead of the elevator.
Make your family outings active, such as a family bike ride or a walk in a park.
If you are sitting for a long time, such as working at a desk or watching TV, do some light activity for 3 minutes or more every half hour.5 Light activities include
leg lifts or extensions
overhead arm stretches
desk chair swivels
torso twists
side lunges
walking in place
Do aerobic exercise
Aerobic exercise is activity that makes your heart beat faster and makes you breathe harder. You should aim for doing aerobic exercise for 30 minutes a day most days of the week. You do not have to do all the activity at one time. You can split up these minutes into a few times throughout the day.
To get the most out of your activity, exercise at a moderate to vigorous level. Try
walking briskly or hiking
climbing stairs
swimming or a water-aerobics class
dancing
riding a bicycle or a stationary bicycle
taking an exercise class
playing basketball, tennis, or other sports
Talk with your health care team about how to warm up and cool down before and after you exercise.
Do strength training to build muscle
Strength training is a light or moderate physical activity that builds muscle and helps keep your bones healthy. Strength training is important for both men and women. When you have more muscle and less body fat, you’ll burn more calories. Burning more calories can help you lose and keep off extra weight.
You can do strength training with hand weights, elastic bands, or weight machines. Try to do strength training two to three times a week. Start with a light weight. Slowly increase the size of your weights as your muscles become stronger.
You can do strength training with hand weights, elastic bands, or weight machines.
Do stretching exercises
Stretching exercises are light or moderate physical activity. When you stretch, you increase your flexibility, lower your stress, and help prevent sore muscles.
You can choose from many types of stretching exercises. Yoga is a type of stretching that focuses on your breathing and helps you relax. Even if you have problems moving or balancing, certain types of yoga can help. For instance, chair yoga has stretches you can do when sitting in a chair or holding onto a chair while standing. Your health care team can suggest whether yoga is right for you.
Having diabetes means that you are more likely to develop heart disease and have a greater chance of a heart attack or a stroke. People with diabetes are also more likely to have certain conditions, or risk factors, that increase the chances of having heart disease or stroke, such as high blood pressure or high cholesterol. If you have diabetes, you can protect your heart and health by managing your blood glucose, also called blood sugar, as well as your blood pressure and cholesterol. If you smoke, get help to stop.
What is the link between diabetes, heart disease, and stroke?
Over time, high blood glucose from diabetes can damage your blood vessels and the nerves that control your heart and blood vessels. The longer you have diabetes, the higher the chances that you will develop heart disease.1
People with diabetes tend to develop heart disease at a younger age than people without diabetes. In adults with diabetes, the most common causes of death are heart disease and stroke. Adults with diabetes are nearly twice as likely to die from heart disease or stroke as people without diabetes.2
What else increases my chances of heart disease or stroke if I have diabetes?
If you have diabetes, other factors add to your chances of developing heart disease or having a stroke.
Smoking
Smoking raises your risk of developing heart disease. If you have diabetes, it is important to stop smoking because both smoking and diabetes narrow blood vessels. Smoking also increases your chances of developing other long-term problems such as lung disease. Smoking also can damage the blood vessels in your legs and increase the risk of lower leg infections, ulcers, and amputation.
High blood pressure
If you have high blood pressure , your heart must work harder to pump blood. High blood pressure can strain your heart, damage blood vessels, and increase your risk of heart attack, stroke, eye problems, and kidney problems.
Abnormal cholesterol levels
Cholesterol is a type of fat produced by your liver and found in your blood. You have two kinds of cholesterol in your blood: LDL and HDL.
LDL, often called “bad” cholesterol, can build up and clog your blood vessels. High levels of LDL cholesterol raise your risk of developing heart disease.
Another type of blood fat, triglycerides, also can raise your risk of heart disease when the levels are higher than recommended by your health care team.
Obesity and belly fat
Being overweight or obese can affect your ability to manage your diabetes and increase your risk for many health problems, including heart disease and high blood pressure. If you are overweight, a healthy eating plan with reduced calories often will lower your glucose levels and reduce your need for medications.
Excess belly fat around your waist, even if you are not overweight, can raise your chances of developing heart disease.
Even if you are a normal weight, excess belly fat can raise your risk for heart disease.
A family history of heart disease may also add to your chances of developing heart disease. If one or more of your family members had a heart attack before age 50, you may have an even higher chance of developing heart disease.3
You can’t change whether heart disease runs in your family, but if you have diabetes, it’s even more important to take steps to protect yourself from heart disease and decrease your chances of having a stroke.
How can I lower my chances of a heart attack or stroke if I have diabetes?
Taking care of your diabetes is important to help you take care of your heart. You can lower your chances of having a heart attack or stroke by taking the following steps to manage your diabetes to keep your heart and blood vessels healthy.
Manage your diabetes ABCs
Knowing your diabetes ABCs will help you manage your blood glucose, blood pressure, and cholesterol. Stopping smoking if you have diabetes is also important to lower your chances for heart disease.
A is for the A1C test. The A1C test shows your average blood glucose level over the past 3 months. This is different from the blood glucose checks that you do every day. The higher your A1C number, the higher your blood glucose levels have been during the past 3 months. High levels of blood glucose can harm your heart, blood vessels, kidneys, feet, and eyes.
The A1C goal for many people with diabetes is below 7 percent. Some people may do better with a slightly higher A1C goal. Ask your health care team what your goal should be.
B is for blood pressure. Blood pressure is the force of your blood against the wall of your blood vessels. If your blood pressure gets too high, it makes your heart work too hard. High blood pressure can cause a heart attack or stroke and damage your kidneys and eyes.
The blood pressure goal for most people with diabetes is below 140/90 mm Hg. Ask what your goal should be.
C is for cholesterol. You have two kinds of cholesterol in your blood: LDL and HDL. LDL or “bad” cholesterol can build up and clog your blood vessels. Too much bad cholesterol can cause a heart attack or stroke. HDL or “good” cholesterol helps remove the “bad” cholesterol from your blood vessels.
Ask your health care team what your cholesterol numbers should be. If you are over 40 years of age, you may need to take medicine such as a statin to lower your cholesterol and protect your heart. Some people with very high LDL (“bad”) cholesterol may need to take medicine at a younger age.
S is for stop smoking. Not smoking is especially important for people with diabetes because both smoking and diabetes narrow blood vessels, so your heart has to work harder.
If you quit smoking
you will lower your risk for heart attack, stroke, nerve disease, kidney disease, eye disease, and amputation
your blood glucose, blood pressure, and cholesterol levels may improve
your blood circulation will improve
you may have an easier time being physically active
If you smoke or use other tobacco products, stop. Ask for help so you don’t have to do it alone. You can start by calling the national quitline at 1-800-QUITNOW or 1-800-784-8669. For tips on quitting, go to Smokefree.gov .
Ask your health care team about your goals for A1C, blood pressure, and cholesterol, and what you can do to reach these goals.
Managing diabetes is not always easy. Feeling stressed, sad, or angry is common when you are living with diabetes. You may know what to do to stay healthy but may have trouble sticking with your plan over time. Long-term stress can raise your blood glucose and blood pressure, but you can learn ways to lower your stress. Try deep breathing, gardening, taking a walk, doing yoga, meditating, doing a hobby, or listening to your favorite music. Learn more about healthy ways to cope with stress .
Take medicine to protect your heart
Medicines may be an important part of your treatment plan. Your doctor will prescribe medicine based on your specific needs. Medicine may help you
meet your A1C (blood glucose), blood pressure, and cholesterol goals.
reduce your risk of blood clots, heart attack, or stroke.
treat angina , or chest pain that is often a symptom of heart disease. (Angina can also be an early symptom of a heart attack.)
Ask your doctor whether you should take aspirin. Aspirin is not safe for everyone. Your doctor can tell you whether taking aspirin is right for you and exactly how much to take.
Statins can reduce the risk of having a heart attack or stroke in some people with diabetes. Statins are a type of medicine often used to help people meet their cholesterol goals. Talk with your doctor to find out whether taking a statin is right for you.
Talk with your doctor if you have questions about your medicines. Before you start a new medicine, ask your doctor about possible side effects and how you can avoid them. If the side effects of your medicine bother you, tell your doctor. Don’t stop taking your medicines without checking with your doctor first.
Take medicines as prescribed.
How do doctors diagnose heart disease in diabetes?
Tests used to monitor your diabetes—A1C, blood pressure, and cholesterol—help your doctor decide whether it is important to do other tests to check your heart health.
Your health care provider will do a physical exam.
What are the warning signs of heart attack and stroke?
Call 9-1-1 right away if you have warning signs of a heart attack:
pain or pressure in your chest that lasts longer than a few minutes or goes away and comes back
pain or discomfort in one or both of your arms or shoulders; or your back, neck, or jaw
shortness of breath
sweating or light-headedness
indigestion or nausea (feeling sick to your stomach)
feeling very tired
Treatment works best when it is given right away. Warning signs can be different in different people. You may not have all of these symptoms.
Call 9-1-1 right away if you have warning signs of a stroke, including sudden
weakness or numbness of your face, arm, or leg on one side of your body
confusion, or trouble talking or understanding
dizziness, loss of balance, or trouble walking
trouble seeing out of one or both eyes
sudden severe headache
If you have any one of these warning signs, call 9-1-1. You can help prevent permanent damage by getting to a hospital within an hour of a stroke.
Call 9-1-1 if you have the warning signs of a heart attack or stroke. Treatment works best when given right away.
Low Blood Glucose (Hypoglycemia)
What is hypoglycemia?
Hypoglycemia, also called low blood glucose or low blood sugar, occurs when the level of glucose in your blood drops below normal. For many people with diabetes, that means a level of 70 milligrams per deciliter (mg/dL) or less. Your numbers might be different, so check with your health care provider to find out what level is too low for you.
What are the symptoms of hypoglycemia?
Symptoms of hypoglycemia tend to come on quickly and can vary from person to person. You may have one or more mild-to-moderate symptoms listed in the table below. Sometimes people don’t feel any symptoms.
Severe hypoglycemia is when your blood glucose level becomes so low that you’re unable to treat yourself and need help from another person. Severe hypoglycemia is dangerous and needs to be treated right away. This condition is more common in people with type 1 diabetes.
Hypoglycemia Symptoms
Mild-to-Moderate
Severe
Shaky or jittery
Sweaty
Hungry
Headachy
Blurred vision
Sleepy or tired
Dizzy or lightheaded
Confused or disoriented
Pale
Uncoordinated
Irritable or nervous
Argumentative or combative
Changed behavior or personality
Trouble concentrating
Weak
Fast or irregular heart beat
Unable to eat or drink
Seizures or convulsions (jerky movements)
Unconsciousness
Some symptoms of hypoglycemia during sleep are
crying out or having nightmares
sweating enough to make your pajamas or sheets damp
feeling tired, irritable, or confused after waking up
What causes hypoglycemia in diabetes?
Hypoglycemia can be a side effect of insulin or other types of diabetes medicines that help your body make more insulin. Two types of diabetes pills can cause hypoglycemia: sulfonylureas and meglitinides. Ask your health care team if your diabetes medicine can cause hypoglycemia.
Although other diabetes medicines don’t cause hypoglycemia by themselves, they can increase the chances of hypoglycemia if you also take insulin, a sulfonylurea, or a meglitinide.
If you take insulin or some other diabetes medicines, your blood glucose level can drop too low.
What other factors contribute to hypoglycemia in diabetes?
If you take insulin or diabetes medicines that increase the amount of insulin your body makes—but don’t match your medications with your food or physical activity—you could develop hypoglycemia. The following factors can make hypoglycemia more likely:
Not eating enough carbohydrates (carbs)
When you eat foods containing carbohydrates, your digestive system breaks down the sugars and starches into glucose. Glucose then enters your bloodstream and raises your blood glucose level. If you don’t eat enough carbohydrates to match your medication, your blood glucose could drop too low.
Skipping or delaying a meal
If you skip or delay a meal, your blood glucose could drop too low. Hypoglycemia also can occur when you are asleep and haven’t eaten for several hours.
Increasing physical activity
Increasing your physical activity level beyond your normal routine can lower your blood glucose level for up to 24 hours after the activity.
Drinking too much alcohol without enough food
Alcohol makes it harder for your body to keep your blood glucose level steady, especially if you haven’t eaten in a while. The effects of alcohol can also keep you from feeling the symptoms of hypoglycemia, which may lead to severe hypoglycemia.
How can I prevent hypoglycemia if I have diabetes?
If you are taking insulin, a sulfonylurea, or a meglitinide, using your diabetes management plan and working with your health care team to adjust your plan as needed can help you prevent hypoglycemia. The following actions can also help prevent hypoglycemia:
Check blood glucose levels
Knowing your blood glucose level can help you decide how much medicine to take, what food to eat, and how physically active to be. To find out your blood glucose level, check yourself with a blood glucose meter as often as your doctor advises.
Hypoglycemia unawareness. Sometimes people with diabetes don’t feel or recognize the symptoms of hypoglycemia, a problem called hypoglycemia unawareness. If you have had hypoglycemia without feeling any symptoms, you may need to check your blood glucose more often so you know when you need to treat your hypoglycemia or take steps to prevent it. Be sure to check your blood glucose before you drive.
If you have hypoglycemia unawareness or have hypoglycemia often, ask your health care provider about a continuous glucose monitor (CGM). A CGM checks your blood glucose level at regular times throughout the day and night. CGMs can tell you if your blood glucose is falling quickly and sound an alarm if your blood glucose falls too low. CGM alarms can wake you up if you have hypoglycemia during sleep.
Eat regular meals and snacks
Your meal plan is key to preventing hypoglycemia. Eat regular meals and snacks with the correct amount of carbohydrates to help keep your blood glucose level from going too low. Also, if you drink alcoholic beverages, it’s best to eat some food at the same time.
Be physically active safely
Physical activity can lower your blood glucose during the activity and for hours afterward. To help prevent hypoglycemia, you may need to check your blood glucose before, during, and after physical activity and adjust your medicine or carbohydrate intake. For example, you might eat a snack before being physically active or decrease your insulin dose as directed by your health care provider to keep your blood glucose from dropping too low.
Work with your health care team
Tell your health care team if you have had hypoglycemia. Your health care team may adjust your diabetes medicines or other aspects of your management plan. Learn about balancing your medicines, eating plan, and physical activity to prevent hypoglycemia. Ask if you should have a glucagon emergency kit to carry with you at all times.
You can help prevent hypoglycemia by working with your health care team.
How do I treat hypoglycemia?
If you begin to feel one or more hypoglycemia symptoms, check your blood glucose. If your blood glucose level is below your target or less than 70, eat or drink 15 grams of carbohydrates right away. Examples include
1/2 cup (4 ounces) of fruit juice—not low-calorie or reduced sugar*
1/2 can (4 to 6 ounces) of soda—not low-calorie or reduced sugar
1 tablespoon of sugar, honey, or corn syrup
2 tablespoons of raisins
Wait 15 minutes and check your blood glucose again. If your glucose level is still low, eat or drink another 15 grams of glucose or carbohydrates. Check your blood glucose again after another 15 minutes. Repeat these steps until your glucose level is back to normal.
If your next meal is more than 1 hour away, have a snack to keep your blood glucose level in your target range. Try crackers or a piece of fruit.
*People who have kidney disease shouldn’t drink orange juice for their 15 grams of carbohydrates because it contains a lot of potassium. Apple, grape, or cranberry juice are good options.
If your blood glucose is below your target, take 15 grams of glucose or carbohydrates right away.
Treating hypoglycemia if you take acarbose or miglitol
If you take acarbose or miglitol along with diabetes medicines that can cause hypoglycemia, you will need to take glucose tablets or glucose gel if your blood glucose level is too low. Eating or drinking other sources of carbohydrates won’t raise your blood glucose level quickly enough.
What if I have severe hypoglycemia and can’t treat myself?
Someone will need to give you a glucagon injection if you have severe hypoglycemia. An injection of glucagon will quickly raise your blood glucose level. Talk with your health care provider about when and how to use a glucagon emergency kit. If you have an emergency kit, check the date on the package to make sure it hasn’t expired.
If you are likely to have severe hypoglycemia, teach your family, friends, and coworkers when and how to give you a glucagon injection. Also, tell your family, friends, and coworkers to call 911 right away after giving you a glucagon injection or if you don’t have a glucagon emergency kit with you.
If you have hypoglycemia often or have had severe hypoglycemia, you should wear a medical alert bracelet or pendant. A medical alert ID tells other people that you have diabetes and need care right away. Getting prompt care can help prevent the serious problems that hypoglycemia can cause.
Autonomic neuropathy is damage to nerves that control your internal organs, leading to problems with your heart rate and blood pressure, digestive system, bladder, sex organs, sweat glands, and eyes. The damage can also lead to hypoglycemia unawareness.
Proximal Neuropathy
Proximal neuropathy is a rare and disabling type of nerve damage in your hip, buttock, or thigh. The damage typically affects one side of your body and may rarely spread to the other side. Symptoms gradually improve over a period of months or years.
Focal Neuropathies
Focal neuropathies are conditions in which you typically have damage to single nerves, most often in your hand, head, torso, or leg. The most common types of focal neuropathy are entrapment syndromes, such as carpal tunnel syndrome. Other types of focal neuropathy are much less common.
What Is Diabetic Neuropathy?
Diabetic neuropathy is nerve damage that is caused by diabetes. Over time, high blood glucose levels, also called blood sugar, and high levels of fats, such as triglycerides, in the blood from diabetes can damage your nerves. Symptoms depend on which type of diabetic neuropathy you have.
Peripheral Neuropathy
Peripheral neuropathy is a type of nerve damage that typically affects the feet and legs and sometimes affects the hands and arms. This type of neuropathy is very common. About one-third to one-half of people with diabetes have peripheral neuropathy.
Diabetes is the leading cause of kidney disease. About 1 out of 4 adults with diabetes has kidney disease.1
The main job of the kidneys is to filter wastes and extra water out of your blood to make urine. Your kidneys also help control blood pressure and make hormones that your body needs to stay healthy.
Your kidneys are located in the middle of your back, just below your rib cage.
When your kidneys are damaged, they can’t filter blood like they should, which can cause wastes to build up in your body. Kidney damage can also cause other health problems.
Kidney damage caused by diabetes usually occurs slowly, over many years. You can take steps to protect your kidneys and to prevent or delay kidney damage.
What increases my chances of developing diabetic kidney disease?
Having diabetes for a longer time increases the chances that you will have kidney damage. If you have diabetes, you are more likely to develop kidney disease if your
blood glucose is too high
blood pressure is too high
African Americans, American Indians, and Hispanics/Latinos develop diabetes, kidney disease, and kidney failure at a higher rate than Caucasians.
You are also more likely to develop kidney disease if you have diabetes and
If you have diabetes, you are more likely to develop kidney disease if you have high blood pressure.
How can I tell if I have diabetic kidney disease?
Most people with diabetic kidney disease do not have symptoms. The only way to know if you have diabetic kidney disease is to get your kidneys checked.
Health care professionals use blood and urine tests to check for diabetic kidney disease. Your health care professional will check your urine for albumin and will also do a blood test to see how well your kidneys are filtering your blood.
You should get tested every year for kidney disease if you
Health care professionals use blood and urine tests to check for kidney disease.
How can I keep my kidneys healthy if I have diabetes?
The best way to slow or prevent diabetes-related kidney disease is to try to reach your blood glucose and blood pressure goals. Healthy lifestyle habits and taking your medicines as prescribed can help you achieve these goals and improve your health overall.
Reach your blood glucose goals
Your health care professional will test your A1C. The A1C is a blood test that shows your average blood glucose level over the past 3 months. This is different from the blood glucose checks that you may do yourself. The higher your A1C number, the higher your blood glucose levels have been during the past 3 months.
The A1C goal for many people with diabetes is below 7 percent. Ask your health care team what your goal should be. Reaching your goal numbers will help you protect your kidneys.
To reach your A1C goal, your health care professional may ask you to check your blood glucose levels. Work with your health care team to use the results to guide decisions about food, physical activity, and medicines. Ask your health care team how often you should check your blood glucose level.
Protect your kidneys by keeping your blood glucose under control.
Control your blood pressure
Blood pressure is the force of your blood against the wall of your blood vessels. High blood pressure makes your heart work too hard. It can cause heart attack, stroke, and kidney disease.
Your health care team will also work with you to help you set and reach your blood pressure goal. The blood pressure goal for most people with diabetes is below 140/90 mm Hg. Ask your health care team what your goal should be.
Protect your kidneys by keeping your blood pressure under control.
Medicines that lower blood pressure can also help slow kidney damage. Two types of blood pressure medicines, ACE inhibitors and ARBs, play a special role in protecting your kidneys. Each has been found to slow kidney damage in people with diabetes who have high blood pressure and DKD. The names of these medicines end in –pril or –sartan. ACE inhibitors and ARBs are not safe for women who are pregnant.
Develop or maintain healthy lifestyle habits
Healthy lifestyle habits can help you reach your blood glucose and blood pressure goals. Following the steps below will also help you keep your kidneys healthy:
Stop smoking.
Work with a dietitian to develop a diabetes meal plan and limit salt and sodium.
Make physical activity part of your routine.
Stay at or get to a healthy weight.
Get enough sleep. Aim for 7 to 8 hours of sleep each night.
Medicines may be an important part of your treatment plan. Your health care professional will prescribe medicine based on your specific needs. Medicine can help you meet your blood glucose and blood pressure goals. You may need to take more than one kind of medicine to control your blood pressure.
Talk to your health care professional or pharmacist about all of the medicines you take, including over-the-counter medicines.
How can I cope with the stress of managing my diabetes?
Managing diabetes isn’t always easy. Feeling stressed, sad, or angry is common when you are living with diabetes. You may know what to do to stay healthy but may have trouble sticking with your plan over time. Long-term stress can raise your blood glucose and blood pressure, but you can learn ways to lower your stress. Try deep breathing, gardening, taking a walk, doing yoga, meditating, doing a hobby, or listening to your favorite music. Learn more about healthy ways to cope with stress .
Does diabetic kidney disease get worse over time?
Kidney damage from diabetes can get worse over time. However, you can take steps to keep your kidneys healthy and help slow kidney damage to prevent or delay kidney failure. Kidney failure means that your kidneys have lost most of their ability to function—less than 15 percent of normal kidney function. However, most people with diabetes and kidney disease don’t end up with kidney failure.
If your kidneys become damaged as a result of diabetes, learn how to manage kidney disease.
References
Diabetes & Foot Problems
Foot problems are common in people with diabetes. You might be afraid you’ll lose a toe, foot, or leg to diabetes, or know someone who has, but you can lower your chances of having diabetes-related foot problems by taking care of your feet every day. Managing your blood glucose levels, also called blood sugar, can also help keep your feet healthy.
How can diabetes affect my feet?
Over time, diabetes may cause nerve damage, also called diabetic neuropathy, that can cause tingling and pain, and can make you lose feeling in your feet. When you lose feeling in your feet, you may not feel a pebble inside your sock or a blister on your foot, which can lead to cuts and sores. Cuts and sores can become infected.
Diabetes also can lower the amount of blood flow in your feet. Not having enough blood flowing to your legs and feet can make it hard for a sore or an infection to heal. Sometimes, a bad infection never heals. The infection might lead to gangrene.
Gangrene and foot ulcers that do not get better with treatment can lead to an amputation of your toe, foot, or part of your leg. A surgeon may perform an amputation to prevent a bad infection from spreading to the rest of your body, and to save your life. Good foot care is very important to prevent serious infections and gangrene.
Although rare, nerve damage from diabetes can lead to changes in the shape of your feet, such as Charcot’s foot. Charcot’s foot may start with redness, warmth, and swelling. Later, bones in your feet and toes can shift or break, which can cause your feet to have an odd shape, such as a “rocker bottom.”
Charcot’s foot can cause your feet to have an odd shape, such as a “rocker bottom.”
What can I do to keep my feet healthy?
Work with your health care team to make a diabetes self-care plan, which is an action plan for how you will manage your diabetes. Your plan should include foot care. A foot doctor, also called a podiatrist, and other specialists may be part of your health care team.
Include these steps in your foot care plan:
Check your feet every day
You may have foot problems, but feel no pain in your feet. Checking your feet each day will help you spot problems early before they get worse. A good way to remember is to check your feet each evening when you take off your shoes. Also check between your toes. If you have trouble bending over to see your feet, try using a mirror to see them, or ask someone else to look at your feet.
Look for problems such as
cuts, sores, or red spots
swelling or fluid-filled blisters
ingrown toenails, in which the edge of your nail grows into your skin
corns or calluses, which are spots of rough skin caused by too much rubbing or pressure on the same spot
plantar warts, which are flesh-colored growths on the bottom of the feet
If you have certain foot problems that make it more likely you will develop a sore on your foot, your doctor may recommend taking the temperature of the skin on different parts of your feet. A “hot spot” can be the first sign that a blister or an ulcer is starting.
Cover a blister, cut, or sore with a bandage. Smooth corns and calluses as explained below.
Wash your feet every day
Wash your feet with soap in warm, not hot, water. Test the water to make sure it is not too hot. You can use a thermometer (90° to 95° F is safe) or your elbow to test the warmth of the water. Do not soak your feet because your skin will get too dry.
After washing and drying your feet, put talcum powder or cornstarch between your toes. Skin between the toes tends to stay moist. Powder will keep the skin dry to help prevent an infection.
Smooth corns and calluses gently
Thick patches of skin called corns or calluses can grow on the feet. If you have corns or calluses, talk with your foot doctor about the best way to care for these foot problems. If you have nerve damage, these patches can become ulcers.
If your doctor tells you to, use a pumice stone to smooth corns and calluses after bathing or showering. A pumice stone is a type of rock used to smooth the skin. Rub gently, only in one direction, to avoid tearing the skin.
Do NOT
cut corns and calluses
use corn plasters, which are medicated pads
use liquid corn and callus removers
Cutting and over-the counter corn removal products can damage your skin and cause an infection.
To keep your skin smooth and soft, rub a thin coat of lotion, cream, or petroleum jelly on the tops and bottoms of your feet. Do not put lotion or cream between your toes because moistness might cause an infection.
Trim your toenails straight across
Trim your toenails, when needed, after you wash and dry your feet. Using toenail clippers, trim your toenails straight across. Do not cut into the corners of your toenail. Gently smooth each nail with an emery board or nonsharp nail file. Trimming this way helps prevent cutting your skin and keeps the nails from growing into your skin.
Have a foot doctor trim your toenails if
you cannot see, feel, or reach your feet
your toenails are thick or yellowed
your nails curve and grow into the skin
If you want to get a pedicure at a salon, you should bring your own nail tools to prevent getting an infection. You can ask your health care provider what other steps you can take at the salon to prevent infection.
Wear shoes and socks at all times
Wear shoes and socks at all times. Do not walk barefoot or in just socks – even when you are indoors. You could step on something and hurt your feet. You may not feel any pain and may not know that you hurt yourself.
Check the inside of your shoes before putting them on, to make sure the lining is smooth and free of pebbles or other objects.
Make sure you wear socks, stockings, or nylons with your shoes to keep from getting blisters and sores. Choose clean, lightly padded socks that fit well. Socks with no seams are best.
Wear shoes that fit well and protect your feet. Here are some tips for finding the right type of shoes:
Walking shoes and athletic shoes are good for daily wear. They support your feet and allow them to “breathe.”
Do not wear vinyl or plastic shoes, because they do not stretch or “breathe.”
When buying shoes, make sure they feel good and have enough room for your toes. Buy shoes at the end of the day, when your feet are the largest, so that you can find the best fit.
If you have a bunion, or hammertoes, which are toes that curl under your feet, you may need extra-wide or deep shoes.1 Do not wear shoes with pointed toes or high heels, because they put too much pressure on your toes.
If your feet have changed shape, such as from Charcot’s foot, you may need special shoes or shoe inserts, called orthotics. You also may need inserts if you have bunions, hammertoes, or other foot problems.
When breaking in new shoes, only wear them for a few hours at first and then check your feet for areas of soreness.
Medicare Part B insurance and other health insurance programs may help pay for these special shoes or inserts. Ask your insurance plan if it covers your special shoes or inserts.
Protect your feet from hot and cold
If you have nerve damage from diabetes, you may burn your feet and not know you did. Take the following steps to protect your feet from heat:
Wear shoes at the beach and on hot pavement.
Put sunscreen on the tops of your feet to prevent sunburn.
Keep your feet away from heaters and open fires.
Do not put a hot water bottle or heating pad on your feet.
Wear socks in bed if your feet get cold. In the winter, wear lined, waterproof boots to keep your feet warm and dry.
Keep the blood flowing to your feet
Try the following tips to improve blood flow to your feet:
Put your feet up when you are sitting.
Wiggle your toes for a few minutes throughout the day. Move your ankles up and down and in and out to help blood flow in your feet and legs.
Do not wear tight socks or elastic stockings. Do not try to hold up loose socks with rubber bands.
Be more physically active. Choose activities that are easy on your feet, such as walking, dancing, yoga or stretching, swimming, or bike riding.
Stop smoking.
Smoking can lower the amount of blood flow to your feet. If you smoke, ask for help to stop. You can get help by calling the national quitline at 1-800-QUITNOW or 1-800-784-8669. For tips on quitting, go to SmokeFree.gov .
Get a foot check at every health care visit
Ask your health care team to check your feet at each visit. Take off your shoes and socks when you’re in the exam room so they will remember to check your feet. At least once a year, get a thorough foot exam, including a check of the feeling and pulses in your feet.
Get a thorough foot exam at each health care visit if you have
Ask your health care team to show you how to care for your feet.
When should I see my health care provider about foot problems?
Call your health care provider right away if you have
a cut, blister, or bruise on your foot that does not start to heal after a few days
skin on your foot that becomes red, warm, or painful—signs of a possible infection
a callus with dried blood inside of it,which often can be the first sign of a wound under the callus
a foot infection that becomes black and smelly—signs you might have gangrene
Ask your provider to refer you to a foot doctor, or podiatrist, if needed.
References
Diabetic Eye Disease
What is diabetic eye disease?
Diabetic eye disease is a group of eye problems that can affect people with diabetes. These conditions include diabetic retinopathy, diabetic macular edema, cataracts, and glaucoma.
Over time, diabetes can cause damage to your eyes that can lead to poor vision or even blindness. But you can take steps to prevent diabetic eye disease, or keep it from getting worse, by taking care of your diabetes.
The best ways to manage your diabetes and keep your eyes healthy are to
Photo courtesy of the National Eye Institute, NIH.
Your eyes may seem fine, but having a full, dilated eye exam is the only way to know for sure.
Often, there are no warning signs of diabetic eye disease or vision loss when damage first develops. A full, dilated eye exam helps your doctor find and treat eye problems early—often before much vision loss can occur.
How does diabetes affect my eyes?
Diabetes affects your eyes when your blood glucose, also called blood sugar, is too high.
In the short term, you are not likely to have vision loss from high blood glucose. People sometimes have blurry vision for a few days or weeks when they’re changing their diabetes care plan or medicines. High glucose can change fluid levels or cause swelling in the tissues of your eyes that help you to focus, causing blurred vision. This type of blurry vision is temporary and goes away when your glucose level gets closer to normal.
If your blood glucose stays high over time, it can damage the tiny blood vessels in the back of your eyes. This damage can begin during prediabetes, when blood glucose is higher than normal, but not high enough for you to be diagnosed with diabetes. Damaged blood vessels may leak fluid and cause swelling. New, weak blood vessels may also begin to grow. These blood vessels can bleed into the middle part of the eye, lead to scarring, or cause dangerously high pressure inside your eye.
Most serious diabetic eye diseases begin with blood vessel problems. The four eye diseases that can threaten your sight are
Diabetic retinopathy
The retina is the inner lining at the back of each eye. The retina senses light and turns it into signals that your brain decodes, so you can see the world around you. Damaged blood vessels can harm the retina, causing a disease called diabetic retinopathy.
In early diabetic retinopathy, blood vessels can weaken, bulge, or leak into the retina. This stage is called nonproliferative diabetic retinopathy.
If the disease gets worse, some blood vessels close off, which causes new blood vessels to grow, or proliferate, on the surface of the retina. This stage is called proliferative diabetic retinopathy. These abnormal new blood vessels can lead to serious vision problems.
Photo courtesy of the National Eye Institute, NIH.
Normal vision of two boys playing.
Photo courtesy of the National Eye Institute, NIH.
Same scene, as viewed by a person with diabetic retinopathy.
Diabetic macular edema
The part of your retina that you need for reading, driving, and seeing faces is called the macula. Diabetes can lead to swelling in the macula, which is called diabetic macular edema. Over time, this disease can destroy the sharp vision in this part of the eye, leading to partial vision loss or blindness. Macular edema usually develops in people who already have other signs of diabetic retinopathy.
Glaucoma
Glaucoma is a group of eye diseases that can damage the optic nerve—the bundle of nerves that connects the eye to the brain. Diabetes doubles the chances of having glaucoma, which can lead to vision loss and blindness if not treated early.
Photo courtesy of the National Eye Institute, NIH.
People with glaucoma slowly lose side vision.
Cataracts
The lenses within our eyes are clear structures that help provide sharp vision—but they tend to become cloudy as we age. People with diabetes are more likely to develop cloudy lenses, called cataracts. People with diabetes can develop cataracts at an earlier age than people without diabetes. Researchers think that high glucose levels cause deposits to build up in the lenses of your eyes.
Photo courtesy of the National Eye Institute, NIH.
Cloudy vision and faded colors are symptoms of cataracts.
How common is diabetic eye disease?
Diabetic retinopathy
About one in three people with diabetes who are older than age 40 already have some signs of diabetic retinopathy.1 Diabetic retinopathy is the most common cause of vision loss in people with diabetes. Each person’s outlook for the future, however, depends in large part on regular care. Finding and treating diabetic retinopathy early can reduce the risk of blindness by 95 percent.
Glaucoma and cataracts
Your chances of developing glaucoma or cataracts are about twice that of someone without diabetes.
Who is more likely to develop diabetic eye disease?
Anyone with diabetes can develop diabetic eye disease. Your risk is greater with
high blood glucose that is not treated
high blood pressure that is not treated
High blood cholesterol and smoking may also raise your risk for diabetic eye disease.
Some groups are affected more than others. African Americans, American Indians and Alaska Natives, Hispanics/Latinos, Pacific Islanders, and older adults are at greater risk of losing vision or going blind from diabetes.
If you have diabetes and become pregnant, you can develop eye problems very quickly during your pregnancy. If you already have some diabetic retinopathy, it can get worse during pregnancy. Changes that help your body support a growing baby may put stress on the blood vessels in your eyes. Your health care team will suggest regular eye exams during pregnancy to catch and treat problems early and protect your vision.
Diabetes that occurs only during pregnancy, called gestational diabetes, does not usually cause eye problems. Researchers aren't sure why this is the case.
Your chances of developing diabetic eye disease increase the longer you have diabetes.
What are the symptoms of diabetic eye disease?
Often there are no early symptoms of diabetic eye disease. You may have no pain and no change in your vision as damage begins to grow inside your eyes, particularly with diabetic retinopathy.
When symptoms do occur, they may include
blurry or wavy vision
frequently changing vision—sometimes from day to day
dark areas or vision loss
poor color vision
spots or dark strings (also called floaters)
flashes of light
Talk with your eye doctor if you have any of these symptoms.
When should I see a doctor right away?
Call a doctor right away if you notice sudden changes to your vision, including flashes of light or many more spots (floaters) than usual. You also should see a doctor right away if it looks like a curtain is pulled over your eyes. These changes in your sight can be symptoms of a detached retina , which is a medical emergency.
How do doctors diagnose eye problems from diabetes?
Having a full, dilated eye exam is the best way to check for eye problems from diabetes. Your doctor will place drops in your eyes to widen your pupils. This allows the doctor to examine a larger area at the back of each eye, using a special magnifying lens. Your vision will be blurry for a few hours after a dilated exam.
Your doctor will also
test your vision
measure the pressure in your eyes
Your doctor may suggest other tests, too, depending on your health history.
Most people with diabetes should see an eye care professional once a year for a complete eye exam. Your own health care team may suggest a different plan, based on your type of diabetes and the time since you were first diagnosed.
How do doctors treat diabetic eye disease?
Your doctor may recommend having eye exams more often than once a year, along with management of your diabetes. This means managing your diabetes ABCs, which include your A1c, blood pressure, and cholesterol; and quitting smoking. Ask your health care team what you can do to reach your goals.
Management of blood glucose can help prevent diabetic eye disease and keep it from getting worse.
Doctors may treat advanced eye problems with medicine, laser treatments, surgery, or a combination of these options.
Medicine
Your doctor may treat your eyes with anti-VEGF medicine, such as aflibercept, bevacizumab, or ranibizumab. These medicines block the growth of abnormal blood vessels in the eye. Anti-VEGF medicines can also stop fluid leaks, which can help treat diabetic macular edema.
The doctor will inject an anti-VEGF medicine into your eyes during office visits. You'll have several treatments during the first few months, then fewer treatments after you finish the first round of therapy. Your doctor will use medicine to numb your eyes so you don’t feel pain. The needle is about the thickness of a human hair.
Anti-VEGF treatments can stop further vision loss and may improve vision in some people.
Laser Treatment
Laser treatment, also called photocoagulation, creates tiny burns inside the eye with a beam of light. This method treats leaky blood vessels and extra fluid, called edema. Your doctor usually provides this treatment during several office visits, using medicine to numb your eyes. Laser treatment can keep eye disease from getting worse, which is important to prevent vision loss or blindness. But laser treatment is less likely to bring back vision you’ve already lost compared with anti-VEGF medicines.
Focal/grid laser treatment works on a small area of the retina to treat diabetic macular edema.
Scatter laser treatment, also called panretinal photocoagulation (PRP), covers a larger area of the retina. This method treats the growth of abnormal blood vessels, called proliferative diabetic retinopathy.
Vitrectomy
Vitrectomy is a surgery to remove the clear gel that fills the center of the eye, called the vitreous gel. The procedure treats problems with severe bleeding or scar tissue caused by proliferative diabetic retinopathy. Scar tissue can force the retina to peel away from the tissue beneath it, like wallpaper peeling away from a wall. A retina that comes completely loose, or detaches, can cause blindness.
During vitrectomy, a clear salt solution is gently pumped into the eye to maintain eye pressure during surgery and to replace the removed vitreous. Vitrectomy is done in a surgery center or hospital with pain medicine.
Cataract Lens Surgery
In a surgery center or hospital visit, your doctor can remove the cloudy lens in your eye, where the cataract has grown, and replace it with an artificial lens. People who have cataract surgery generally have better vision afterward. After your eye heals, you may need a new prescription for your glasses. Your vision following cataract surgery may also depend on treating any damage from diabetic retinopathy or macular edema.
What can I do to protect my eyes?
To prevent diabetic eye disease, or to keep it from getting worse, manage your diabetes ABCs: your A1c, blood pressure, and cholesterol; and quit smoking if you smoke. Read more information on how to manage diabetes.
Also, have a dilated eye exam at least once a year—or more often if recommended by your eye care professional. These actions are powerful ways to protect the health of your eyes—and can prevent blindness.
The sooner you work to manage your diabetes and other health conditions, the better. And, even if you’ve struggled in the past to manage your health, taking better care of yourself now can protect your eyes for the future. It’s never too late to begin.
What if I already have some vision loss from diabetes?
Ask your eye care professional to help you find a low vision and rehabilitation clinic. Special eye care professionals can help you manage vision loss that cannot be corrected with glasses, contact lenses, medicine, or surgery. Special devices and training may help you make the most of your remaining vision so that you can continue to be active, enjoy hobbies, visit friends and family members, and live without help from others.
References:
Diabetes, Gum Disease, & Other Dental Problems
How can diabetes affect my mouth?
Too much glucose, also called sugar, in your blood from diabetes can cause pain, infection, and other problems in your mouth. Your mouth includes
your teeth
your gums
your jaw
tissues such as your tongue, the roof and bottom of your mouth, and the inside of your cheeks
Glucose is present in your saliva—the fluid in your mouth that makes it wet. When diabetes is not controlled, high glucose levels in your saliva help harmful bacteria grow. These bacteria combine with food to form a soft, sticky film called plaque. Plaque also comes from eating foods that contain sugars or starches. Some types of plaque cause tooth decay or cavities. Other types of plaque cause gum disease and bad breath.
Gum disease can be more severe and take longer to heal if you have diabetes. In turn, having gum disease can make your blood glucose hard to control.
What happens if I have plaque?
Plaque that is not removed hardens over time into tartar and collects above your gum line. Tartar makes it more difficult to brush and clean between your teeth. Your gums become red and swollen, and bleed easily—signs of unhealthy or inflamed gums, called gingivitis.
When gingivitis is not treated, it can advance to gum disease called periodontitis. In periodontitis, the gums pull away from the teeth and form spaces, called pockets, which slowly become infected. This infection can last a long time. Your body fights the bacteria as the plaque spreads and grows below the gum line. Both the bacteria and your body’s response to this infection start to break down the bone and the tissue that hold the teeth in place. If periodontitis is not treated, the gums, bones, and tissue that support the teeth are destroyed. Teeth may become loose and might need to be removed. If you have periodontitis, your dentist may send you to a periodontist, an expert in treating gum disease.
Healthy gums Periodontitis
What are the most common mouth problems from diabetes?
The following chart shows the most common mouth problems from diabetes.
Problem
What It Is
Symptoms
Treatment
gingivitis
unhealthy or inflamed gums
red, swollen, and bleeding gums
daily brushing and flossing
regular cleanings at the dentist
periodontitis
gum disease, which can change from mild to severe
red, swollen, and bleeding gums
gums that have pulled away from the teeth
long-lasting infection between the teeth and gums
bad breath that won’t go away
permanent teeth that are loose or moving away from one another
changes in the way your teeth fit together when you bite
sometimes pus between the teeth and gums
changes in the fit of dentures, which are teeth you can remove
deep cleaning at your dentist
medicine that your dentist prescribes
gum surgery in severe cases
thrush, called candidiasis
the growth of a naturally occurring fungus that the body is unable to control
sore, white—or sometimes red—patches on your gums, tongue, cheeks, or the roof of your mouth
patches that have turned into open sores
medicine that your doctor or dentist prescribes to kill the fungus
cleaning dentures
removing dentures for part of the day or night, and soaking them in medicine that your doctor or dentist prescribes
dry mouth, called xerostomia
a lack of saliva in your mouth, which raises your risk for tooth decay and gum disease
dry feeling in your mouth, often or all of the time
dry, rough tongue
pain in the mouth
cracked lips
mouth sores or infection
problems chewing, eating, swallowing, or talking
taking medicine to keep your mouth wet that your doctor or dentist prescribes
rinsing with a fluoride mouth rinse to prevent cavities
using sugarless gum or mints to increase saliva flow
taking frequent sips of water
avoiding tobacco, caffeine, and alcoholic beverages
using a humidifier, a device that raises the level of moisture in your home, at night
avoiding spicy or salty foods that may cause pain in a dry mouth
oral burning
a burning sensation inside the mouth caused by uncontrolled blood glucose levels
burning feeling in the mouth
dry mouth
bitter taste
symptoms may worsen throughout the day
seeing your doctor, who may change your diabetes medicine
once your blood glucose is under control, the oral burning will go away
More symptoms of a problem in your mouth are
a sore, or an ulcer, that does not heal
dark spots or holes in your teeth
pain in your mouth, face, or jaw that doesn’t go away
loose teeth
pain when chewing
a changed sense of taste or a bad taste in your mouth
bad breath that doesn’t go away when you brush your teeth
How will I know if I have mouth problems from diabetes?
Check your mouth for signs of problems from diabetes. If you notice any problems, see your dentist right away. Some of the first signs of gum disease are swollen, tender, or bleeding gums. Sometimes you won’t have any signs of gum disease. You may not know you have it until you have serious damage. Your best defense is to see your dentist twice a year for a cleaning and checkup.
Check your mouth for signs of problems from diabetes.
How can I prepare for a visit to my dentist?
Plan ahead. Talk with your doctor and dentist before the visit about the best way to take care of your blood glucose during dental work.
You may be taking a diabetes medicine that can cause low blood glucose, also called hypoglycemia. If you take insulin or other diabetes medicines, take them and eat as usual before visiting the dentist. You may need to bring your diabetes medicines and your snacks or meal with you to the dentist’s office.
You may need to postpone any nonemergency dental work if your blood glucose is not under control.
If you feel nervous about visiting the dentist, tell your dentist and the staff about your feelings. Your dentist can adapt the treatment to your needs. Don’t let your nerves stop you from having regular checkups. Waiting too long to take care of your mouth may make things worse.
If you feel nervous about visiting the dentist, tell your dentist and the staff about your feelings.
What if my mouth is sore after my dental work?
A sore mouth is common after dental work. If this happens, you might not be able to eat or chew the foods you normally eat for several hours or days. For guidance on how to adjust your usual routine while your mouth is healing, ask your doctor
what foods and drinks you should have
if you should change the time when you take your diabetes medicines
if you should change the dose of your diabetes medicines
Smoking makes problems with your mouth worse. Smoking raises your chances of getting gum disease, oral and throat cancers, and oral fungal infections. Smoking also discolors your teeth and makes your breath smell bad.
Smoking and diabetes are a dangerous mix. Smoking raises your risk for many diabetes problems. If you quit smoking,
your cholesterol and blood pressure levels might improve
your blood circulation will improve
If you smoke, stop smoking. Ask for help so that you don’t have to do it alone. You can start by calling 1–800–QUITNOW or 1–800–784–8669.
How can I keep my mouth healthy?
You can keep your mouth healthy by taking these steps:
Keep your blood glucose numbers as close to your target as possible. Your doctor will help you set your target blood glucose numbers and teach you what to do if your numbers are too high or too low.
Eat healthy meals and follow the meal plan that you and your doctor or dietitian have worked out.
Brush your teeth at least twice a day with fluoride toothpaste. Fluoride protects against tooth decay.
Aim for brushing first thing in the morning, before going to bed, and after each meal and sugary or starchy snack.
Use a soft toothbrush.
Gently brush your teeth with the toothbrush angled towards the gum line.
Use small, circular motions.
Brush the front, back, and top of each tooth. Brush your tongue, too.
Change your toothbrush every 3 months or sooner if the toothbrush looks worn or the bristles spread out. A new toothbrush removes more plaque.
Drink water that contains added fluoride or ask your dentist about using a fluoride mouth rinse to prevent tooth decay.
Ask your dentist about using an anti-plaque or anti-gingivitis mouth rinse to control plaque or prevent gum disease.
Use dental floss to clean between your teeth at least once a day. Flossing helps prevent plaque from building up on your teeth. When flossing,
slide the floss up and down and then curve it around the base of each tooth under the gums
use clean sections of floss as you move from tooth to tooth
Another way of removing plaque between teeth is to use a dental pick or brush—thin tools designed to clean between the teeth. You can buy these picks at drug stores or grocery stores.
If you wear dentures, keep them clean and take them out at night. Have them adjusted if they become loose or uncomfortable.
Call your dentist right away if you have any symptoms of mouth problems.
See your dentist twice a year for a cleaning and checkup. Your dentist may suggest more visits if you need them.
See your dentist twice a year for a cleaning and checkup.
Follow your dentist’s advice.
If your dentist tells you about a problem, take care of it right away.
Follow any steps or treatments from your dentist to keep your mouth healthy.
Tell your dentist that you have diabetes.
Tell your dentist about any changes in your health or medicines.
Share the results of some of your diabetes blood tests, such as the A1C test or the fasting blood glucose test.
Ask if you need antibiotics before and after dental treatment if your diabetes is uncontrolled.
If you smoke, stop smoking.
Diabetes, Sexual, & Bladder Problems
Sexual problems and bladder problems are common as people age, but diabetes can make these problems worse. You or your partner may have trouble having or enjoying sex. Or, you may leak urine or have trouble emptying your bladder normally.
Blood vessels and nerves can be damaged by the effects of high blood glucose, also called blood sugar. This damage can lead to sexual and bladder problems. Keeping your blood glucose levels in your target range is an important way to prevent damage to your blood vessels and nerves.
Work with your health care team to help prevent or treat sexual and bladder problems. These problems may be signs that you need to manage your diabetes in a different way. Remember, a healthy sex life and a healthy bladder can improve your quality of life, so take action now if you have concerns.
Sexual and bladder problems may be signs that you need to manage your diabetes in a different way.
Can sexual and bladder problems be symptoms of diabetes?
Yes. Changes in sexual function or bladder habits may be a sign that you have diabetes. Nerve damage caused by diabetes, also called diabetic neuropathy, can damage parts of your body—like your genitals or urinary tract. For example, men with diabetes may develop erectile dysfunction (ED) 10 to 15 years earlier than men without diabetes.1
Talk with a health care professional if you have any symptoms of diabetes, including sexual and bladder problems.
When should I see a doctor about my sexual or bladder problems?
See a health care professional for problems with sex or your bladder. These problems could be a sign that you need to manage your diabetes differently. You may find it embarrassing and difficult to talk about these things. However, remember that health care professionals are trained to speak with people about every kind of health problem. Everyone deserves to have healthy relationships and enjoy the activities they love.
What makes me more likely to develop sexual or bladder problems?
You’re more likely to develop sexual or bladder problems if you have diabetes and
have high blood glucose that is not well controlled, also called high blood sugar
Research also suggests that certain genes may make people more likely to develop diabetic neuropathy.2
What sexual problems can men with diabetes have?
Changes in your blood vessels, nerves, hormones, and emotional health during diabetes may make it more difficult for you to have satisfactory sex. Diabetes and its related challenges also may make it harder for you to have a child.
Erectile dysfunction
You have ED if you’re unable to get or keep an erection firm enough for satisfactory sexual intercourse. More than half of men with diabetes will get ED. Men who have diabetes are more than 3 times more likely to develop ED than men who do not have diabetes.1Good diabetes management may help prevent and treat ED caused by nerve damage and circulation problems. A doctor can help treat ED with medicine or a change in your diabetes care plan.
Managing your diabetes may help prevent and treat ED caused by nerve damage and circulation problems.
Retrograde ejaculation
Rarely, diabetes can cause retrograde ejaculation , which is when part or all of your semen goes into your bladder instead of out of your penis during ejaculation. During retrograde ejaculation, semen enters your bladder, mixes with urine, and is safely urinated out. A urine sample after ejaculation can show if you have retrograde ejaculation. Some men with retrograde ejaculation may not ejaculate at all.
Penile curvature
Men with diabetes are more likely to have Peyronie’s disease, also called penile curvature, than men who don’t have diabetes.3 Men with Peyronie’s disease have scar tissue, called a plaque, in the penis, making it curve when erect. Curves in the penis can make sexual intercourse painful or difficult. Some men with Peyronie’s disease may have ED.
Low testosterone
Men’s testosterone levels naturally lower with age. However, lower-than-normal testosterone levels may be the cause of some men’s ED, or can explain why some men often feel tired, depressed , or have a low sex drive. Men with diabetes, especially those who are older and overweight, are more likely to have low testosterone , or “low T.”
If your doctor thinks you might have low T, you will probably be asked to give a blood sample, and a health care professional will give you a physical exam. Your doctor may suggest treating your low testosterone with a prescription gel, injection, or patch.
Several studies show that, along with good diabetes management, testosterone therapy can lessen a man’s sexual problems.4 However, testosterone therapy may have serious risks and may not be safe for all men. Talk with your doctor about testosterone therapy’s side effects and whether it’s right for you.
Fertility problems
Some studies show that men with diabetes can have problems with their sperm that make it harder to conceive. Your sperm could be slow or not move well, or your sperm may not be able to fertilize a woman’s egg well.5 Working closely with your partner and a health care professional trained in fertility issues may help.
If you and your partner want to conceive a child, your doctor may treat retrograde ejaculation caused by diabetes with medicine or by changing your diabetes care plan. Or, talk with a urologist who is a fertility expert. He or she may be able to collect your sperm from your urine and then use it for artificial insemination .
What sexual problems can women with diabetes have?
Low sexual desire and response, vaginal dryness, and painful sex can be caused by nerve damage, reduced blood flow to the genitals, and hormonal changes. Other conditions can cause these problems, too, including menopause . If you notice a change in your sex life, talk with your health care team. A physical exam, which will include a pelvic exam, and blood and urine tests may help your doctor find the cause of your problems.
Low sexual desire and response
Low sexual desire and sexual response can include
being unable to become or stay aroused
not having enough vaginal lubrication
having little to no feeling in your genitals
being unable to have an orgasm or rarely having one
With diabetes, your body and mind will likely go through many changes. For example, both high and low blood glucose levels can affect how and if you become aroused. Or, you may find yourself more tired than usual or depressed and anxious , making you less interested in sex.
Your health care team can help you make changes to your diabetes care plan so that you‘re back on track. Women who keep blood glucose levels in their target range are less likely to have nerve damage, which can lead to low sexual desire and response.
Painful sex
Some women with diabetes say they have uncomfortable or painful sexual intercourse. The nerves that tell your vagina to lubricate during stimulation can become damaged by diabetes. A prescription or over-the-counter vaginal lubricant may help if you have vaginal dryness. Managing your blood glucose well over many weeks, months, and years can help prevent nerve damage.
Yeast and bladder infections
Women with diabetes are more likely to have yeast infections , because yeast organisms can grow more easily when your blood glucose levels are higher. Yeast infections can be uncomfortable or painful and prevent you from enjoying activities, including having sex.
Although some yeast infections can be treated at home, talk with a health care professional first about your symptoms. Some symptoms of yeast infections are similar to other types of infections, including sexually transmitted diseases.
Pregnancy concerns and fertility problems
If you have diabetes and plan to become pregnant, it’s important to get your blood glucose levels close to your target range before you get pregnant. High blood glucose can harm your baby during the first weeks of pregnancy, even before you know you’re pregnant.
If you have diabetes and are already pregnant, see your doctor as soon as possible to make a plan to manage your diabetes. Working with your health care team and following your diabetes management plan can help you have a healthy pregnancy and a healthy baby.
Conditions such as obesity and polycystic ovarian syndrome (PCOS) that are linked to diabetes can make it harder to conceive a child. Talk with a health care professional, such as a gynecologist or a fertility specialist, if you’re having problems conceiving a child.
If you notice a change in your sex life, talk with your health care team.
What bladder problems can men and women with diabetes have?
Diabetes can cause nerve damage to your urinary tract, causing bladder problems. Overweight and obesity also can increase bladder problems, such as urinary incontinence (UI). Managing diabetes is an important part of preventing problems that can lead to excess urination.
Your health care team may be able to help you manage your blood glucose levels and help you lose weight, if needed. Doctors use blood and urine tests to diagnose bladder problems or conditions with similar symptoms. Doctors also may use urodynamic testing to see what kind of bladder problem you have.
Frequent and urgent urination
Some people with diabetes who regularly have high blood glucose levels may have to urinate too often, also called urinary frequency. Even men and women with diabetes who manage their blood glucose levels within their target range sometimes feel the sudden urge to urinate, called urgency incontinence. This can happen at night, also. Medicines may help reduce the symptoms of bladder control problems.
Trouble “going”
You may find that diabetes causes you to no longer feel when your bladder is full. Many people with diabetes report that they have trouble “going.” Over time, having a too-full bladder can cause damage to your bladder muscles that push urine out. When these muscles don’t work correctly, urine may stay in your bladder too long, also called urinary retention. Urinary retention can cause bladder infections, urine leaks, and the feeling that you always have to go.
Leaking urine
People with diabetes are more likely to have other types of UI, such as stress incontinence. Nerve damage, obesity, and bladder infections, which are linked with diabetes, are often related to bladder control problems. Leaking urine can cause you to avoid activities you once enjoyed, including sex.
If you’re overweight, losing weight can help you have fewer leaks. Avoiding weight gain may prevent UI. Studies suggest that, as your body mass index (BMI) increases, you’re more likely to leak.6 If you’re overweight or have obesity, talk with your doctor about how to lose weight.
Work with your health care team to help manage and prevent urine leaks. Bladder control problems are often treatable and are very common, even in people who don’t have diabetes. You don’t have to accept rushing to the bathroom all the time to avoid leaks.
Bladder infections
People with diabetes are more likely to have urinary tract infections, also called bladder infections, or cystitis. See a doctor right away if you have frequent, urgent urination that may be painful. Bladder infections can develop into kidney infections and can make bladder symptoms, such as leaks and urine retention, worse. Also, bladder infections can get in the way of your everyday life, including intimacy. Managing your blood glucose levels can help prevent bladder infections.
Managing your blood glucose levels can help prevent bladder problems.
How can I prevent and treat my sexual or bladder problems?
Managing your diabetes can help prevent nerve damage and other diabetes problems that can lead to sexual and bladder problems. With your health care team, you can help prevent and treat your sexual or bladder control problems by
keeping your blood glucose, blood pressure, and cholesterol levels close to your target numbers
getting help for any emotional or psychological problems
Sex is a physical activity, so be sure to check your blood glucose level before and after sex, especially if you take insulin. Both high blood glucose levels and low blood glucose levels can cause problems during sex.
Counseling may also be helpful when you notice changes in your sexual function or desire. These types of changes are very common as people age or adjust to health problems.
If you have a partner, he or she also may be an important member of your health care team. You may find it helpful to share your concerns and have that person join you at the doctor’s office or at counseling. Your friends and family may also be able to support you if you’re having bladder problems.