Diabetes occurs when your blood glucose, also called blood sugar, is too high. Blood glucose is your main source of energy and comes mainly from the food you eat. Insulin, a hormone made by the pancreas, helps the glucose in your blood get into your cells to be used for energy. Another hormone, glucagon, works with insulin to control blood glucose levels.
In most people with type 1 diabetes, the body’s immune system, which normally fights infection, attacks and destroys the cells in the pancreas that make insulin. As a result, your pancreas stops making insulin. Without insulin, glucose can’t get into your cells and your blood glucose rises above normal. People with type 1 diabetes need to take insulin every day to stay alive.
People with type 1 diabetes need to take insulin every day.
Who is more likely to develop type 1 diabetes?
Type 1 diabetes typically occurs in children and young adults, although it can appear at any age. Having a parent or sibling with the disease may increase your chance of developing type 1 diabetes. In the United States, about 5 percent of people with diabetes have type 1.1
What are the symptoms of type 1 diabetes?
Symptoms of type 1 diabetes are serious and usually happen quickly, over a few days to weeks. Symptoms can include
increased thirst and urination
increased hunger
blurred vision
fatigue
unexplained weight loss
Sometimes the first symptoms of type 1 diabetes are signs of a life-threatening condition called diabetic ketoacidosis (DKA) . Some symptoms of DKA include
DKA is serious and dangerous. If you or your child have symptoms of DKA, contact your health care professional right away, or go to the nearest hospital emergency room.
What causes type 1 diabetes?
Experts think type 1 diabetes is caused by genes and factors in the environment, such as viruses, that might trigger the disease. Researchers are working to pinpoint the causes of type 1 diabetes through studies such as TrialNet .
How do health care professionals diagnose type 1 diabetes?
Health care professionals usually test people for type 1 diabetes if they have clear-cut diabetes symptoms. Health care professionals most often use the random plasma glucose (RPG) test to diagnose type 1 diabetes. This blood test measures your blood glucose level at a single point in time. Sometimes health professionals also use the A1C blood test to find out how long someone has had high blood glucose.
Even though these tests can confirm that you have diabetes, they can’t identify what type you have. Treatment depends on the type of diabetes, so knowing whether you have type 1 or type 2 is important.
To find out if your diabetes is type 1, your health care professional may test your blood for certain autoantibodies. Autoantibodies are antibodies that attack your healthy tissues and cells by mistake. The presence of certain types of autoantibodies is common in type 1 but not in type 2 diabetes.
Because type 1 diabetes can run in families, your health care professional can test your family members for autoantibodies. Type 1 diabetes TrialNet, an international research network, also offers autoantibody testing to family members of people diagnosed with the disease. The presence of autoantibodies, even without diabetes symptoms, means the family member is more likely to develop type 1 diabetes. If you have a brother or sister, child, or parent with type 1 diabetes, you may want to get an autoantibody test. People age 20 or younger who have a cousin, aunt, uncle, niece, nephew, grandparent, or half-sibling with type 1 diabetes also may want to get tested.
What medicines do I need to treat my type 1 diabetes?
If you have type 1 diabetes, you must take insulin because your body no longer makes this hormone. Different types of insulin start to work at different speeds, and the effects of each last a different length of time. You may need to use more than one type. You can take insulin a number of ways. Common options include a needle and syringe, insulin pen, or insulin pump.
Some people who have trouble reaching their blood glucose targets with insulin alone also might need to take another type of diabetes medicine that works with insulin, such as pramlintide . Pramlintide, given by injection, helps keep blood glucose levels from going too high after eating. Few people with type 1 diabetes take pramlintide, however. The NIH has recently funded a large research study to test use of pramlintide along with insulin and glucagon in people with type 1 diabetes. Another diabetes medicine, metformin, may help decrease the amount of insulin you need to take, but more studies are needed to confirm this. Reseachers are also studying other diabetes pills that people with type 1 diabetes might take along with insulin.
Hypoglycemia, or low blood sugar, can occur if you take insulin but don’t match your dose with your food or physical activity. Severe hypoglycemia can be dangerous and needs to be treated right away. Learn more about hypoglycemia and how to prevent or treat it.
How else can I manage type 1 diabetes?
Along with insulin and any other medicines you use, you can manage your diabetes by taking care of yourself each day. Following your diabetes meal plan, being physically active, and checking your blood glucose often are some of the ways you can take care of yourself. Work with your health care team to come up with a diabetes care plan that works for you. If you are planning a pregnancy with diabetes, try to get your blood glucose levels in your target range before you get pregnant.
Do I have other treatment options for my type 1 diabetes?
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) has played an important role in developing “artificial pancreas” technology. An artificial pancreas replaces manual blood glucose testing and the use of insulin shots. A single system monitors blood glucose levels around the clock and provides insulin or a combination of insulin and glucagon automatically. The system can also be monitored remotely, for example by parents or medical staff.
In 2016, the U.S. Food and Drug Administration approved a type of artificial pancreas system called a hybrid closed-loop system. This system tests your glucose level every 5 minutes throughout the day and night through a continuous glucose monitor, and automatically gives you the right amount of basal insulin, a long-atcing insulin, through a separate insulin pump. You still need to manually adjust the amount of insulin the pump delivers at mealtimes and when you need a correction dose. You also will need to test your blood with a glucose meter several times a day. Talk with your health care provider about whether this system might be right for you.
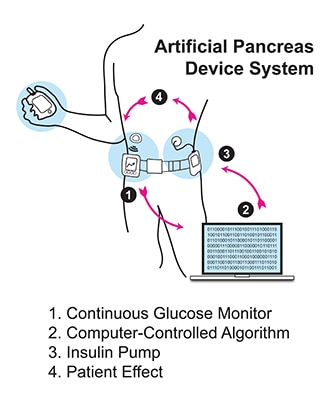
The illustration below shows the parts of a type of artificial pancreas system.
An artificial pancreas system uses a continuous glucose monitor, an insulin pump, and a control algorithm to give you the right amount of basal insulin.
The continuous glucose monitor sends information through a software program called a control algorithm. Based on your glucose level, the algorithm tells the insulin pump how much insulin to deliver. The software program could be installed on the pump or another device such as a cell phone or computer.
Starting in late 2016 and early 2017, the NIDDK has funded several important studies on different types of artificial pancreas devices to better help people with type 1 diabetes manage their disease. The devices may also help people with type 2 diabetes and gestational diabetes.
NIDDK is also supporting research into pancreatic islet transplantation—an experimental treatment for hard-to-control type 1 diabetes. Pancreatic islets are clusters of cells in the pancreas that make insulin. Type 1 diabetes attacks these cells. A pancreatic islet transplant replaces destroyed islets with new ones that make and release insulin. This procedure takes islets from the pancreas of an organ donor and transfers them to a person with type 1 diabetes. Because researchers are still studying pancreatic islet transplantation, the procedure is only available to people enrolled in a study. Learn more about islet transplantation studies .
What health problems can people with type 1 diabetes develop?
Over time, high blood glucose leads to problems such as
Can I lower my chance of developing type 1 diabetes?
At this time, type 1 diabetes can’t be prevented. However, through studies such as TrialNet, researchers are working to identify possible ways to prevent or slow down the disease.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
Rita Basu, M.D., Mayo Clinic
Type 2 Diabetes
What is type 2 diabetes?
Type 2 diabetes, the most common type of diabetes, is a disease that occurs when your blood glucose, also called blood sugar, is too high. Blood glucose is your main source of energy and comes mainly from the food you eat. Insulin, a hormone made by the pancreas, helps glucose get into your cells to be used for energy. In type 2 diabetes, your body doesn’t make enough insulin or doesn’t use insulin well. Too much glucose then stays in your blood, and not enough reaches your cells.
The good news is that you can take steps to prevent or delay the development of type 2 diabetes.
Who is more likely to develop type 2 diabetes?
You can develop type 2 diabetes at any age, even during childhood. However, type 2 diabetes occurs most often in middle-aged and older people. You are more likely to develop type 2 diabetes if you are age 45 or older, have a family history of diabetes, or are overweight or obese. Diabetes is more common in people who are African American, Hispanic/Latino, American Indian, Asian American, or Pacific Islander.
Type 2 diabetes occurs most often in middle-aged and older people.
What are the symptoms of diabetes?
Symptoms of diabetes include
increased thirst and urination
increased hunger
feeling tired
blurred vision
numbness or tingling in the feet or hands
sores that do not heal
unexplained weight loss
Symptoms of type 2 diabetes often develop slowly—over the course of several years—and can be so mild that you might not even notice them. Many people have no symptoms. Some people do not find out they have the disease until they have diabetes-related health problems, such as blurred vision or heart disease.
What causes type 2 diabetes?
Type 2 diabetes is caused by several factors, including
How do health care professionals diagnose type 2 diabetes?
Your health care professional can diagnose type 2 diabetes based on blood tests. Learn more about blood tests for diabetes and what the results mean.
How can I manage my type 2 diabetes?
Managing your blood glucose, blood pressure, and cholesterol, and quitting smoking if you smoke, are important ways to manage your type 2 diabetes. Lifestyle changes that include planning healthy meals, limiting calories if you are overweight, and being physically active are also part of managing your diabetes. So is taking any prescribed medicines. Work with your health care team to create a diabetes care plan that works for you.
Following your meal plan helps you manage your diabetes.
What medicines do I need to treat my type 2 diabetes?
Along with following your diabetes care plan, you may need diabetes medicines, which may include pills or medicines you inject under your skin, such as insulin. Over time, you may need more than one diabetes medicine to manage your blood glucose. Even if you don’t take insulin, you may need it at special times, such as during pregnancy or if you are in the hospital. You also may need medicines for high blood pressure, high cholesterol, or other conditions.
What health problems can people with diabetes develop?
Following a good diabetes care plan can help protect against many diabetes-related health problems. However, if not managed, diabetes can lead to problems such as
Many people with type 2 diabetes also have nonalcoholic fatty liver disease (NAFLD). Losing weight if you are overweight or obese can improve NAFLD. Diabetes is also linked to other health problems such as sleep apnea, depression, some types of cancer, and dementia .
How can I lower my chances of developing type 2 diabetes?
Research such as the Diabetes Prevention Program , sponsored by the National Institutes of Health, has shown that you can take steps to reduce your chances of developing type 2 diabetes if you have risk factors for the disease. Here are some things you can do to lower your risk:
Lose weight if you are overweight, and keep it off. You may be able to prevent or delay diabetes by losing 5 to 7 percent of your current weight.1 For instance, if you weigh 200 pounds, your goal would be to lose about 10 to 14 pounds.
Move more. Get at least 30 minutes of physical activity, such as walking, at least 5 days a week. If you have not been active, talk with your health care professional about which activities are best. Start slowly and build up to your goal.
Eat healthy foods. Eat smaller portions to reduce the amount of calories you eat each day and help you lose weight. Choosing foods with less fat is another way to reduce calories. Drink water instead of sweetened beverages.
Ask your health care team what other changes you can make to prevent or delay type 2 diabetes.
Most often, your best chance for preventing type 2 diabetes is to make lifestyle changes that work for you long term. Get started with Your Game Plan to Prevent Type 2 Diabetes.
The NIDDK would like to thank:
Rita Basu, M.D., Mayo Clinic
Insulin Resistance & Prediabetes
Insulin resistance and prediabetes occur when your body doesn’t use insulin well.
What is insulin?
Insulin is a hormone made by the pancreas that helps glucose in your blood enter cells in your muscle, fat, and liver, where it’s used for energy. Glucose comes from the food you eat. The liver also makes glucose in times of need, such as when you’re fasting. When blood glucose, also called blood sugar, levels rise after you eat, your pancreas releases insulin into the blood. Insulin then lowers blood glucose to keep it in the normal range.
What is insulin resistance?
Insulin resistance is when cells in your muscles, fat, and liver don’t respond well to insulin and can’t easily take up glucose from your blood. As a result, your pancreas makes more insulin to help glucose enter your cells. As long as your pancreas can make enough insulin to overcome your cells’ weak response to insulin, your blood glucose levels will stay in the healthy range.
What is prediabetes?
Prediabetes means your blood glucose levels are higher than normal but not high enough to be diagnosed as diabetes. Prediabetes usually occurs in people who already have some insulin resistance or whose beta cells in the pancreas aren’t making enough insulin to keep blood glucose in the normal range. Without enough insulin, extra glucose stays in your bloodstream rather than entering your cells. Over time, you could develop type 2 diabetes.
How common is prediabetes?
More than 84 million people ages 18 and older have prediabetes in the United States.1 That’s about 1 out of every 3 adults.
Who is more likely to develop insulin resistance or prediabetes?
People who have genetic or lifestyle risk factors are more likely to develop insulin resistance or prediabetes. Risk factors include
People who have metabolic syndrome—a combination of high blood pressure, abnormal cholesterol levels, and large waist size—are more likely to have prediabetes.
Along with these risk factors, other things that may contribute to insulin resistance include
Although you can’t change risk factors such as family history, age, or ethnicity, you can change lifestyle risk factors around eating, physical activity, and weight. These lifestyle changes can lower your chances of developing insulin resistance or prediabetes.
Being overweight or having obesity are risk factors for developing insulin resistance or prediabetes.
What causes insulin resistance and prediabetes?
Researchers don’t fully understand what causes insulin resistance and prediabetes, but they think excess weight and lack of physical activity are major factors.
Excess weight
Experts believe obesity, especially too much fat in the abdomen and around the organs, called visceral fat, is a main cause of insulin resistance. A waist measurement of 40 inches or more for men and 35 inches or more for women is linked to insulin resistance. This is true even if your body mass index (BMI) falls within the normal range. However, research has shown that Asian Americans may have an increased risk for insulin resistance even without a high BMI.
Researchers used to think that fat tissue was only for energy storage. However, studies have shown that belly fat makes hormones and other substances that can contribute to chronic, or long-lasting, inflammation in the body. Inflammation may play a role in insulin resistance, type 2 diabetes, and cardiovascular disease.
Excess weight may lead to insulin resistance, which in turn may play a part in the development of fatty liver disease.
Physical inactivity
Not getting enough physical activity is linked to insulin resistance and prediabetes. Regular physical activity causes changes in your body that make it better able to keep your blood glucose levels in balance.
What are the symptoms of insulin resistance and prediabetes?
Insulin resistance and prediabetes usually have no symptoms. Some people with prediabetes may have darkened skin in the armpit or on the back and sides of the neck, a condition called acanthosis nigricans. Many small skin growths called skin tags often appear in these same areas.
Even though blood glucose levels are not high enough to cause symptoms for most people, a few research studies have shown that some people with prediabetes may already have early changes in their eyes that can lead to retinopathy. This problem more often occurs in people with diabetes.
How do doctors diagnose insulin resistance and prediabetes?
Doctors use blood tests to find out if someone has prediabetes, but they don’t usually test for insulin resistance. The most accurate test for insulin resistance is complicated and used mostly for research.
Doctors use blood tests to find out if someone has prediabetes.
Doctors most often use the fasting plasma glucose (FPG) test or the A1C test to diagnose prediabetes. Less often, doctors use the oral glucose tolerance test (OGTT), which is more expensive and not as easy to give.
The A1C test reflects your average blood glucose over the past 3 months. The FPG and OGTT show your blood glucose level at the time of the test. The A1C test is not as sensitive as the other tests. In some people, it may miss prediabetes that the OGTT could catch. The OGTT can identify how your body handles glucose after a meal—often before your fasting blood glucose level becomes abnormal. Often doctors use the OGTT to check for gestational diabetes, a type of diabetes that develops during pregnancy.
People with prediabetes have up to a 50 percent chance of developing diabetes over the next 5 to 10 years. You can take steps to manage your prediabetes and prevent type 2 diabetes.
The following test results show Prediabetes2
A1C—5.7 to 6.4 percent
FPG—100 to 125 mg/dL (milligrams per deciliter)
OGTT—140 to 199 mg/dL
You should be tested for prediabetes if you are overweight or have obesity and have one or more other risk factors for diabetes, or if your parents, siblings, or children have type 2 diabetes. Even if you don’t have risk factors, you should start getting tested once you reach age 45.
If the results are normal but you have other risk factors for diabetes, you should be retested at least every 3 years.2
How can I prevent or reverse insulin resistance and prediabetes?
Physical activity and losing weight if you need to may help your body respond better to insulin. Taking small steps, such as eating healthier foods and moving more to lose weight, can help reverse insulin resistance and prevent or delay type 2 diabetes in people with prediabetes.
Physical activity can help prevent or reverse insulin resistance and prediabetes.
The National Institutes of Health-funded research study, the Diabetes Prevention Program (DPP), showed that for people at high risk of developing diabetes, losing 5 to 7 percent of their starting weight helped reduce their chance of developing the disease.3 That’s 10 to 14 pounds for someone who weighs 200 pounds. People in the study lost weight by changing their diet and being more physically active.
The DPP also showed that taking metformin , a medicine used to treat diabetes, could delay diabetes. Metformin worked best for women with a history of gestational diabetes, younger adults, and people with obesity. Ask your doctor if metformin might be right for you.
Making a plan, tracking your progress, and getting support from your health care professional, family, and friends can help you make lifestyle changes that may prevent or reverse insulin resistance and prediabetes. You may be able to take part in a lifestyle change program as part of the National Diabetes Prevention Program .
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you?
Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you .
What clinical trials are open?
Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov .
References
May 2018
The NIDDK would like to thank Rita Basu, M.D., University of Virginia School of Medicine
Gestational diabetes is a type of diabetes that develops during pregnancy. Diabetes means your blood glucose, also called blood sugar, is too high. Too much glucose in your blood is not good for you or your baby.
Gestational diabetes is usually diagnosed in the 24th to 28th week of pregnancy. Managing your gestational diabetes can help you and your baby stay healthy. You can protect your own and your baby’s health by taking action right away to manage your blood glucose levels.
How can gestational diabetes affect my baby?
High blood glucose levels during pregnancy can cause problems for your baby, such as
being born too early
weighing too much, which can make delivery difficult and injure your baby
having low blood glucose, also called hypoglycemia, right after birth
having breathing problems
High blood glucose also can increase the chance that you will have a miscarriage or a stillborn baby.1 Stillborn means the baby dies in the womb during the second half of pregnancy.
Your baby also will be more likely to become overweight and develop type 2 diabetes as he or she gets older.
How can gestational diabetes affect me?
If you have gestational diabetes, you are more likely to develop preeclampsia, which is when you develop high blood pressure and too much protein in your urine during the second half of pregnancy.
Preeclampsia can cause serious or life-threatening problems for you and your baby. The only cure for preeclampsia is to give birth. If you have preeclampsia and have reached 37 weeks of pregnancy, your doctor may want to deliver your baby early. Before 37 weeks, you and your doctor may consider other options to help your baby develop as much as possible before he or she is born. Learn more about preeclampsia .
Gestational diabetes may increase your chance of having a cesarean section , also called a C-section, because your baby may be large. A C-section is major surgery.
If you have gestational diabetes, you are more likely to develop type 2 diabetes later in life. Over time, having too much glucose in your blood can cause health problems such as diabetic retinopathy, heart disease, kidney disease, and nerve damage. You can take steps to help prevent or delay type 2 diabetes.
References
Symptoms & Causes
What are the symptoms of gestational diabetes?
Usually, gestational diabetes has no symptoms. If you do have symptoms, they may be mild, such as being thirstier than normal or having to urinate more often.
What causes gestational diabetes?
Gestational diabetes occurs when your body can’t make the extra insulin needed during pregnancy. Insulin, a hormone made in your pancreas, helps your body use glucose for energy and helps control your blood glucose levels.
During pregnancy, your body makes special hormones and goes through other changes, such as weight gain. Because of these changes, your body’s cells don’t use insulin well, a condition called insulin resistance. All pregnant women have some insulin resistance during late pregnancy. Most pregnant women can produce enough insulin to overcome insulin resistance, but some cannot. These women develop gestational diabetes.
Pregnant women who can’t make enough insulin during late pregnancy develop gestational diabetes.
Being overweight or obese is linked to gestational diabetes. Women who are overweight or obese may already have insulin resistance when they become pregnant. Gaining too much weight during pregnancy may also be a factor.
Having a family history of diabetes makes it more likely that a woman will develop gestational diabetes, which suggests that genes play a role.
Tests & Diagnosis
When will I be tested for gestational diabetes?
Testing for gestational diabetes usually occurs between 24 and 28 weeks of pregnancy.
Doctors use blood tests to diagnose gestational diabetes. You may have the glucose challenge test, the oral glucose tolerance test, or both. These tests show how well your body uses glucose.
You will have one or more blood tests to check for gestational diabetes.
Glucose Challenge Test
You may have the glucose challenge test first. Another name for this blood test is the glucose screening test. In this test, a health care professional will draw your blood 1 hour after you drink a sweet liquid containing glucose. You do not need to fast for this test. Fasting means having nothing to eat or drink except water. If your blood glucose is too high—140 or more—you may need to return for an oral glucose tolerance test while fasting. If your blood glucose is 200 or more, you may have type 2 diabetes.
Oral Glucose Tolerance Test (OGTT)
The OGTT measures blood glucose after you fast for at least 8 hours. First, a health care professional will draw your blood. Then you will drink the liquid containing glucose. You will need your blood drawn every hour for 2 to 3 hours for a doctor to diagnose gestational diabetes.
High blood glucose levels at any two or more blood test times—fasting, 1 hour, 2 hours, or 3 hours—mean you have gestational diabetes. Your health care team will explain what your OGTT results mean.
Your health care professional may recommend an OGTT without first having the glucose challenge test.
Management & Treatment
How can I manage my gestational diabetes?
Many women with gestational diabetes can manage their blood glucose levels by following a healthy eating plan and being physically active. Some women also may need diabetes medicine.
Follow a healthy eating plan
Your health care team will help you make a healthy eating plan with food choices that are good for you and your baby. The plan will help you know which foods to eat, how much to eat, and when to eat. Food choices, amounts, and timing are all important in keeping your blood glucose levels in your target range.
Your health care team will help you make a healthy eating plan.
If you’re not eating enough or your blood glucose is too high, your body might make ketones. Ketones in your urine or blood mean your body is using fat for energy instead of glucose. Burning large amounts of fat instead of glucose can be harmful to your health and your baby’s health.
Your doctor might recommend you test your urine or blood daily for ketones or when your blood glucose is above a certain level, such as 200. If your ketone levels are high, your doctor may suggest that you change the type or amount of food you eat. Or, you may need to change your meal or snack times.
Be physically active
Physical activity can help you reach your target blood glucose levels. If your blood pressure or cholesterol levels are too high, being physically active can help you reach healthy levels. Physical activity can also relieve stress, strengthen your heart and bones, improve muscle strength, and keep your joints flexible. Being physically active will also help lower your chances of having type 2 diabetes in the future.
Talk with your health care team about what activities are best for you during your pregnancy. Aim for 30 minutes of activity 5 days of the week, even if you weren’t active before your pregnancy.2 If you are already active, tell your doctor what you do. Ask your doctor if you may continue some higher intensity activities, such as lifting weights or jogging.
How will I know whether my blood glucose levels are on target?
Your health care team may ask you to use a blood glucose meter to check your blood glucose levels. This device uses a small drop of blood from your finger to measure your blood glucose level. Your health care team can show you how to use your meter.
Recommended daily target blood glucose levels for most women with gestational diabetes are
Before meals, at bedtime, and overnight: 95 or less
1 hour after eating: 140 or less
2 hours after eating: 120 or less3
Ask your doctor what targets are right for you.
Your health care team may ask you to use a blood glucose meter to check your blood glucose levels.
You can keep track of your blood glucose levels using My Daily Blood Glucose Record (PDF, 45 KB). You can also use an electronic blood glucose tracking system on your computer or mobile device. Record the results every time you check your blood glucose. Your blood glucose records can help you and your health care team decide whether your diabetes care plan is working. Take your tracker with you when you visit your health care team.
How is gestational diabetes treated if diet and physical activity aren’t enough?
If following your eating plan and being physically active aren’t enough to keep your blood glucose levels in your target range, you may need insulin.
If you need to use insulin, your health care team will show you how to give yourself insulin shots. Insulin will not harm your baby and is usually the first choice of diabetes medicine for gestational diabetes. Researchers are studying the safety of the diabetes pills metformin and glyburide during pregnancy, but more long-term studies are needed. Talk with your health care professional about what treatment is right for you.
References
Prevention
What increases my chance of developing gestational diabetes?
Your chance of developing gestational diabetes are higher if you
Being overweight, a family history, or having prediabetes increases your chance of developing gestational diabetes.
How can I lower my chance of developing gestational diabetes?
If you are thinking about becoming pregnant and are overweight, you can lower your chance of developing gestational diabetes by losing extra weight and increasing physical activity before you become pregnant. Taking these steps can improve how your body uses insulin and help your blood glucose levels stay normal.
Once you are pregnant, don’t try to lose weight. You need to gain some weight for your baby to be healthy. However, gaining too much weight too quickly may increase your chance of developing gestational diabetes. Ask your doctor how much weight gain and physical activity during pregnancy are right for you.
After Your Baby is Born
After I have my baby, how can I find out whether I have diabetes?
You should get tested for diabetes no later than 12 weeks after your baby is born. If your blood glucose is still high, you may have type 2 diabetes. Even if your blood glucose is normal, you still have a greater chance of developing type 2 diabetes in the future. Therefore, you should be tested for diabetes every 3 years.
How can I prevent or delay type 2 diabetes later in life?
You can do a lot to prevent or delay type 2 diabetes. Here are steps you should take if you had gestational diabetes:
Be more active and make healthy food choices to get back to a healthy weight.
Breastfeed your baby. Breastfeeding gives your baby the right balance of nutrients and helps you burn calories.
If your test results show that you could get diabetes and you are overweight, ask your doctor about what changes you can make to lose weight and for help in making them. Your doctor may recommend that you take medicine such as metformin to help prevent type 2 diabetes.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
Boyd Metzger, M.D., Northwestern University
The most common forms of diabetes, type 1 and type 2, are polygenic, meaning they are related to a change, or defect, in multiple genes. Environmental factors, such as obesity in the case of type 2 diabetes, also play a part in the development of polygenic forms of diabetes. Polygenic forms of diabetes often run in families. Doctors diagnose polygenic forms of diabetes by testing blood glucose, also known as blood sugar, in individuals with risk factors or symptoms of diabetes.
Genes provide the instructions for making proteins within the cell. If a gene has a change or mutation, the protein may not function properly. Genetic mutations that cause diabetes affect proteins that play a role in the ability of the body to produce insulin or in the ability of insulin to lower blood glucose. People typically have two copies of most genes, with one gene inherited from each parent.
What are monogenic forms of diabetes?
Some rare forms of diabetes result from mutations or changes in a single gene and are called monogenic. In the United States, monogenic forms of diabetes account for about 1 to 4 percent of all cases of diabetes.1,2,3,4 In most cases of monogenic diabetes, the gene mutation is inherited from one or both parents. Sometimes the gene mutation develops spontaneously, meaning that the mutation is not carried by either of the parents. Most mutations that cause monogenic diabetes reduce the body’s ability to produce insulin, a protein produced in the pancreas that helps the body use glucose for energy.
Neonatal diabetes mellitus (NDM) and maturity-onset diabetes of the young (MODY) are the two main forms of monogenic diabetes. NDM occurs in newborns and young infants. MODY is much more common than NDM and usually first occurs in adolescence or early adulthood.
Most cases of monogenic diabetes are incorrectly diagnosed. For example, when high blood glucose is first detected in adulthood, type 2 diabetes is often diagnosed instead of monogenic diabetes. If your health care provider thinks you might have monogenic diabetes, genetic testing may be needed to diagnose it and to identify which type. Testing of other family members may also be indicated to determine whether they are at risk for or already have a monogenic form of diabetes that is passed down from generation to generation. Some monogenic forms of diabetes can be treated with oral diabetes medicines (pills), while other forms require insulin injections. A correct diagnosis allows for proper treatment and can lead to better glucose control and improved health in the long term.
What is neonatal diabetes mellitus (NDM)?
NDM is a monogenic form of diabetes that occurs in the first 6 to 12 months of life. NDM is a rare condition accounting for up to 1 in 400,000 infants in the United States.4 Infants with NDM do not produce enough insulin, leading to an increase in blood glucose. NDM is often mistaken for type 1 diabetes, but type 1 diabetes is very rarely seen before 6 months of age. Diabetes that occurs in the first 6 months of life almost always has a genetic cause. Researchers have identified a number of specific genes and mutations that can cause NDM. In about half of those with NDM, the condition is lifelong and is called permanent neonatal diabetes mellitus (PNDM). In the rest of those with NDM, the condition is transient, or temporary, and disappears during infancy but can reappear later in life. This type of NDM is called transient neonatal diabetes mellitus (TNDM).
Clinical features of NDM depend on the gene mutations a person has. Signs of NDM include frequent urination, rapid breathing, and dehydration.5 NDM can be diagnosed by finding elevated levels of glucose in blood or urine. The lack of insulin may cause the body to produce chemicals called ketones, resulting in a potentially life-threatening condition called diabetic ketoacidosis. Most fetuses with NDM do not grow well in the womb, and newborns with NDM are much smaller than those of the same gestational age, a condition called intrauterine growth restriction. After birth, some infants fail to gain weight and grow as rapidly as other infants of the same age and sex. Appropriate therapy may improve and normalize growth and development.
What is maturity onset diabetes of the young (MODY)?
MODY is a monogenic form of diabetes that usually first occurs during adolescence or early adulthood. MODY accounts for up to 2 percent of all cases of diabetes in the United States in people ages 20 and younger.3
A number of different gene mutations have been shown to cause MODY, all of which limit the ability of the pancreas to produce insulin. This leads to high blood glucose levels and, in time, may damage body tissues, particularly the eyes, kidneys, nerves, and blood vessels.
Clinical features of MODY depend on the gene mutations a person has. People with certain types of mutations may have slightly high blood sugar levels that remain stable throughout life, have mild or no symptoms of diabetes, and do not develop any long-term complications. Their high blood glucose levels may only be discovered during routine blood tests. However, other mutations require specific treatment with either insulin or a type of oral diabetes medication called sulfonylureas.
MODY may be confused with type 1 or type 2 diabetes. In the past, people with MODY have generally not been overweight or obese, or have other risk factors for type 2 diabetes, such as high blood pressure or abnormal blood fat levels. However, as more people in the United States become overweight or obese, people with MODY may also be overweight or obese.
Although both type 2 diabetes and MODY can run in families, people with MODY typically have a family history of diabetes in multiple successive generations, meaning MODY is present in a grandparent, a parent, and a child.
How is monogenic diabetes diagnosed?
Genetic testing can diagnose most forms of monogenic diabetes. A correct diagnosis with proper treatment should lead to better glucose control and improved health in the long term.
Genetic testing is recommended if 6
diabetes is diagnosed within the first 6 months of age
diabetes is diagnosed in children and young adults, particularly those with a strong family history of diabetes, who do not have typical features of type 1 or type 2 diabetes, such as the presence of diabetes-related autoantibodies, obesity, and other metabolic features
a person has stable, mild fasting hyperglycemia, especially if obesity is not present
If you think that you or a member of your family may have a monogenic form of diabetes, talk to your doctor.
What do I need to know about genetic testing and counseling?
Genetic testing for monogenic diabetes involves providing a blood or saliva sample from which DNA is isolated. The DNA is analyzed for changes in the genes that cause monogenic diabetes. Genetic testing is done by specialized labs.
Abnormal results can determine the gene responsible for diabetes in a particular individual or show whether someone is likely to develop a monogenic form of diabetes in the future. Genetic testing can be helpful in selecting the most appropriate treatment for individuals with monogenic diabetes. Testing is also important in planning for pregnancy and to understand the risk of having a child with monogenic diabetes if you, your partner, or your family members have monogenic diabetes.
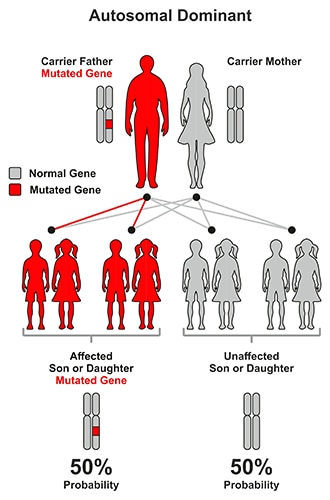
Most forms of NDM and MODY are caused by autosomal dominant mutations, meaning that the condition can be passed on to children when only one parent carries or has the disease gene. With dominant mutations, a parent who carries the gene has a 50 percent chance of having an affected child with monogenic diabetes.
In most forms of MODY, a parent with MODY has a 50 percent chance of having a child with the disease.
In contrast, with autosomal recessive disease, a mutation must be inherited from both parents. In this instance, a child has a 25 percent chance of having monogenic diabetes.
For recessive forms of monogenic diabetes, testing can indicate whether parents or siblings without disease are carriers for recessive genetic conditions that could be inherited by their children.
While not as common, it is possible to inherit mutations from the mother only (X-linked mutations). Also not as common are mutations that occur spontaneously.
When both parents carry autosomal recessive mutations, a child has a 25 percent chance of having (or being affected by) the disease.
More information about the genes that cause NDM and MODY, the types of mutations responsible for the disease (autosomal dominant, autosomal recessive, X-linked, etc.), and clinical features is provided in the American Diabetes Association Standards of Medical Care in Diabetes .
If you suspect that you or a member of your family may have a monogenic form of diabetes, you should seek help from health care professionals—physicians and genetic counselors—who have specialized knowledge and experience in this area. They can determine whether genetic testing is appropriate; select the genetic tests that should be performed; and provide information about the basic principles of genetics, genetic testing options, and confidentiality issues. They also can review the test results with the patient or parent after testing, make recommendations about how to proceed, and discuss testing options for other family members.
How is monogenic diabetes treated and managed?
Treatment varies depending on the specific genetic mutation that has caused a person’s monogenic diabetes. People with certain forms of MODY and NDM can be treated with a sulfonylurea, an oral diabetes medicine that helps the body release more insulin into the blood. Other people may need insulin injections. Some people with MODY may not need medications and are able to manage their diabetes with lifestyle changes alone, which include physical activity and healthy food choices. Your physician and diabetes care team will work with you to develop a plan to treat and manage your diabetes based on the results of genetic testing.
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you?
Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you .
What clinical trials are open?
Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov .
References
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
Louis Philipson, M.D., Ph.D., University of Chicago, Department of Medicine, Endocrinology, Director, Kovler Diabetes Center
Cystic Fibrosis-Related Diabetes
Causes of CFRD
Symptoms, Screening, and Diagnosis
Treating CFRD
Cystic fibrosis-related diabetes (CFRD) is a unique type of diabetes that is common in people with CF. With early diagnosis and proper treatment, CFRD can be managed successfully.
Causes of CFRD
There are two types of diabetes in people without cystic fibrosis. Type 1 diabetes is an autoimmune disease that occurs when the body's immune system attacks and destroys the cells in the pancreas that make insulin (beta cells). Insulin helps the body absorb and use the energy from food. This helps maintain good nutrition and lung function in people with CF.
Type 1 diabetes is most commonly diagnosed in childhood. People with type 1 diabetes need to take insulin to stay alive. Type 2 diabetes occurs more often in adults who are overweight or obese, and is caused by the lack of a normal response to insulin in addition to the pancreas not making enough insulin.
CFRD shares some features with both type 1 and type 2 diabetes. In people with CF, the thick, sticky mucus that is characteristic of the disease causes scarring of the pancreas. This scarring prevents the pancreas from producing normal amounts of insulin, so, like people with type 1 diabetes, they become insulin deficient. Their pancreas still makes some insulin, but not enough to stay healthy and maintain good nutrition.
Additionally, people with CFRD may not respond to insulin in the right way like people with type 2 diabetes, especially when sick, when taking steroid medication, and when pregnant. This is referred to as being "insulin resistant."
Symptoms, Screening, and Diagnosis
People with CFRD may not experience any symptoms. Some diabetes symptoms are similar to other CF symptoms you may already have. Many people with CFRD do not know they have CFRD until they are tested for diabetes.
Some common symptoms, like increased thirst and urination, are caused by high blood sugar levels, known as hyperglycemia. Other symptoms of CFRD are excessive fatigue, weight loss, and unexplained decline in lung function.
The CF care guidelines for CFRD recommend that people with CF ages 10 and older be tested every year for CFRD with an oral glucose tolerance test (OGTT). The OGTT is the best way to diagnose CFRD and is usually done in the morning after an eight-hour fast. If you are diagnosed with CFRD, you will receive proper treatment in order to feel better, gain weight, and improve your lung function.
Listen to Andrea Kelly, M.D., talk about CFRD and what's changed since she's been in the field of CF.
The goal for treating CFRD is to keep blood sugar (glucose) at normal or near-normal levels. Doing so will help you gain weight, maintain muscle mass, feel better, and have more energy. Maintaining normal glucose levels also lowers the risk of problems caused by diabetes.
CFRD can be well managed with insulin, along with monitoring your blood sugar levels, eating your usual high-calorie diet, and staying active.
There are many types of insulin, which are grouped by how fast they work and how long they last in the body. Insulin is injected into the body and helps your body cells absorb the energy (calories) from the food you eat. Calories in food come from carbohydrates, protein, and fat. Insulin helps the body cells absorb these three nutrients so you can achieve and maintain a healthy body weight and good nutritional status.
People with CFRD still need to eat the same high-calorie, high-protein, high-fat, high-salt diet to help achieve and maintain a healthy body weight. Since foods with carbohydrates turn into blood glucose when eaten, people with CFRD need to count the carbohydrates in the foods they eat so they can give themselves the right amount of insulin. Your diabetes care team will help you determine the amount of insulin you need for your carbohydrates.
Physical activity like exercise is good for lung function and can also improve your body's response to insulin. People with CFRD are encouraged to do at least 150 minutes of some type of moderate aerobic exercise -- activities that require you to breathe in oxygen, like jogging or playing sports -- every week. Monitoring your blood sugar levels will allow you to remain active since exercise may cause the levels to drop when muscles use the sugar for energy.
If you are diagnosed with CFRD, your CF care team may expand to include an endocrinologist (a doctor with special training in the treatment of diabetes) and certified diabetes educators. Working with you, this team will design a treatment plan to help you manage your diabetes while also maintaining your health with CF.